
Why the border between uterus, placenta and membranes may matter
A pregnancy hematoma is often described as a blood collection near the gestational sac, membranes or placenta.
That description is correct, but it can sound too simple.
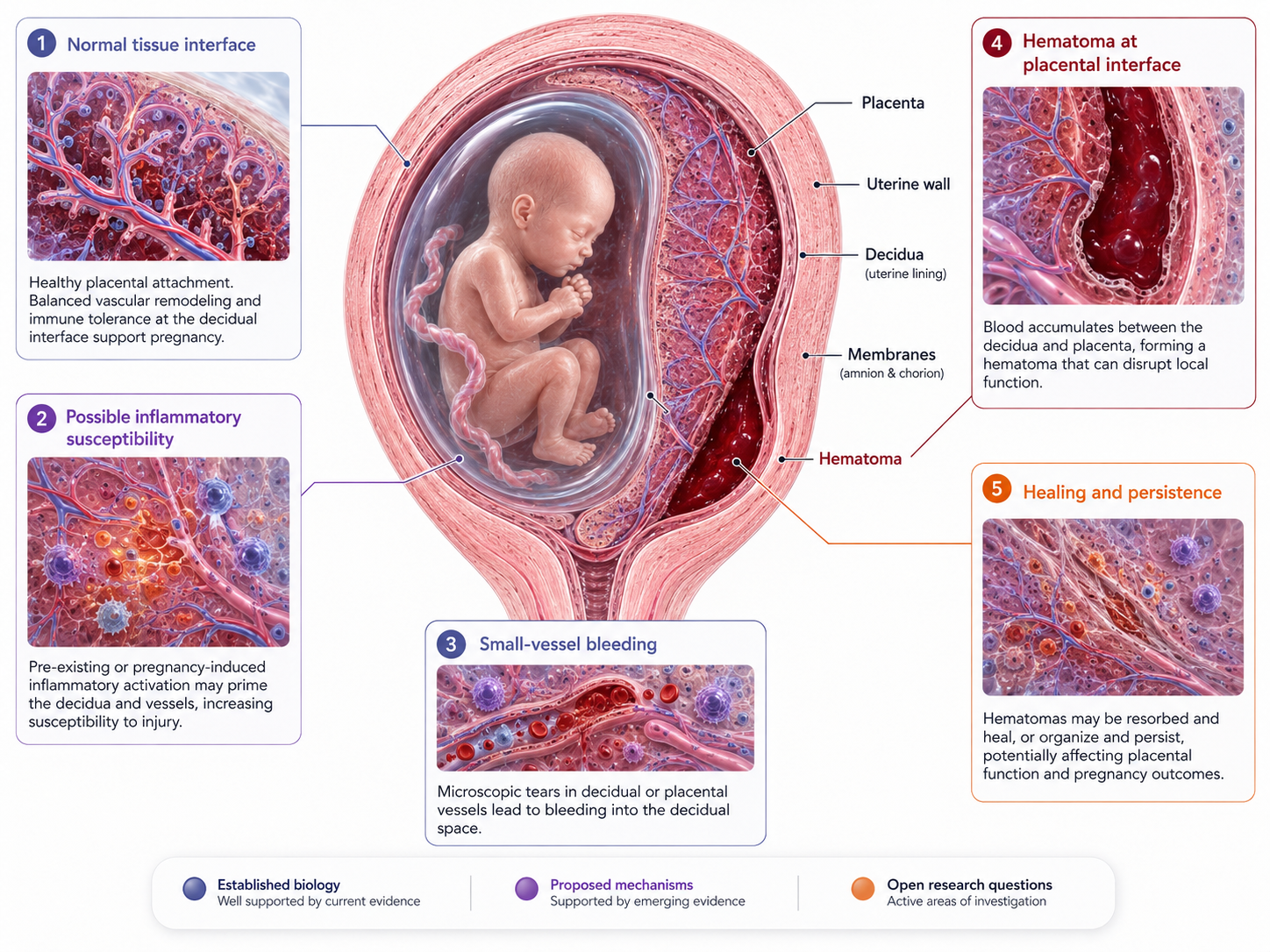
The blood does not appear in empty space. It appears near living tissue interfaces: the uterine lining, decidua, chorionic membrane, placental edge, placental attachment and maternal blood vessels. These tissues are active, vascular, immune-regulated and constantly adapting during pregnancy.
This is why the pregnancy tissue interface matters.
A hematoma may be easier to understand if we ask not only:
Where is the blood?
But also:
What kind of tissue did the bleeding come from?
Was the local tissue fragile?
Was the maternal-fetal interface inflamed?
Was placental attachment normal?
Was the decidual tissue healthy?
Were there underlying conditions such as endometriosis, adenomyosis, IVF history or immune imbalance?
These questions do not prove a cause. But they help explain why hematoma research should not be limited to “blood clot size.”
A hematoma may be a visible sign of a local tissue event.
What is the pregnancy tissue interface?
The pregnancy tissue interface is the region where maternal and pregnancy-derived tissues meet.
This includes:
- the decidua, which is the pregnancy-adapted uterine lining
- the chorion and other gestational membranes
- the placental attachment area
- maternal blood vessels supplying the placenta
- immune cells that help regulate pregnancy tolerance and tissue remodeling
- the uterine wall beneath the implantation site
This interface must do something biologically difficult.
It must allow the placenta to attach, grow and communicate with maternal circulation, while also maintaining immune tolerance, vascular stability and tissue integrity.
It is not passive tissue.
It is a highly regulated biological zone.
Why inflammation could matter
Inflammation is not always bad. Controlled immune activity is part of normal implantation, placental development and tissue remodeling.
But excessive, chronic or poorly regulated inflammation may affect tissue behavior.
At the pregnancy tissue interface, inflammation could theoretically influence:
- vascular fragility
- local bleeding tendency
- decidual stability
- placental attachment
- immune cell activation
- tissue repair
- clot breakdown and remodeling
- communication between placenta and uterine lining
This does not mean that every hematoma is caused by inflammation.
It means inflammation may be one possible contributor in some cases, especially when there is a relevant background such as endometriosis, adenomyosis, recurrent pregnancy loss, IVF history or other inflammatory conditions.
The challenge is that this is difficult to prove in an individual pregnancy.
A visible hematoma does not tell us exactly why the vessel bled.
Decidua: more than just “uterine lining”
Before pregnancy, the endometrium changes during the menstrual cycle. After implantation, it transforms into decidua.
The decidua is not just a lining. It is an active pregnancy tissue.
It helps regulate:
- implantation
- placental development
- maternal immune tolerance
- vascular remodeling
- tissue support around the gestational sac
- communication between maternal and fetal-derived tissues
If the decidual environment is abnormal, inflamed or structurally altered, it is biologically plausible that the interface could become more vulnerable.
This is one reason why conditions affecting the endometrium or uterine environment are interesting in hematoma research.
But again, this remains a research question.
A patient should not be told that her hematoma is definitely caused by “bad decidua” or “inflammation” unless there is specific evidence in her case.
Endometriosis as a possible context
Endometriosis is an inflammatory condition where endometrial-like tissue exists outside the uterus. It is associated with chronic inflammatory signaling, altered immune responses and, in many women, fertility challenges.
Research has associated endometriosis with several adverse pregnancy outcomes, including preterm birth, placenta previa, placental abruption, hypertensive disorders, cesarean delivery and stillbirth in some studies. This does not mean every woman with endometriosis will have complications, but it does suggest that endometriosis may influence pregnancy biology beyond pain and fertility.
The direct relationship between endometriosis and pregnancy hematoma is less clear.
This distinction is important.
What can be said carefully:
Endometriosis is associated with altered inflammatory and reproductive biology.
Endometriosis has been linked in research to some placental and pregnancy complications.
It is biologically plausible that inflammatory or decidual changes could contribute to bleeding risk in some pregnancies.
A direct causal pathway from endometriosis to pregnancy hematoma is not established for every case.
This is exactly the type of question that belongs in applied research.
IVF, implantation and the tissue interface
IVF pregnancies are often monitored more closely, which means hematomas may be detected more often. Detection bias may play a role: if you scan more, you may find more.
At the same time, IVF pregnancies can differ from spontaneous pregnancies in background factors. These may include infertility diagnosis, endometriosis, uterine factors, maternal age, hormonal preparation, embryo transfer conditions and early pregnancy monitoring patterns.
This makes interpretation complicated.
If a hematoma is found after IVF, it may not be caused by IVF itself. It may relate to underlying infertility factors, implantation biology, placental development, medication context or simply closer ultrasound surveillance.
For research, IVF pregnancies can be valuable because they often have detailed early data. But for an individual patient, overinterpretation should be avoided.
The placenta and vascular fragility
Placental development requires controlled invasion and remodeling of maternal vessels.
If this process is disrupted, local blood vessels may be more fragile or the tissue interface may be less stable.
Some reviews of subchorionic hematoma discuss possible mechanisms involving trophoblast invasion, angiogenesis, vascular fragility and early placental development. These mechanisms are plausible because hematoma formation requires bleeding somewhere in the local tissue environment.
However, the field is not settled.
Studies differ. Definitions vary. Hematomas are measured differently. Some are symptomatic, others are incidental. Some occur early, others persist into later pregnancy. Some are small and peripheral, others are larger or closer to the placenta.
This is why one universal explanation is unlikely.
Pregnancy hematoma is probably not one single condition with one single cause.
It may be a shared ultrasound finding with different underlying mechanisms.
Could inflammation affect clearance as well as formation?
Inflammation may be relevant not only to why bleeding starts, but also to how tissue heals afterward.
Once blood collects, the body must stabilize the clot, break it down, remove blood products and remodel the tissue space.
This process involves immune cells, local vessels and tissue repair pathways.
In theory, an altered inflammatory environment could affect:
- how quickly the clot organizes
- how efficiently blood products are cleared
- whether tissue remains irritated
- whether spotting continues
- whether the hematoma persists
- how the interface remodels over time
This is plausible, but not yet a proven clinical model for individual pregnancies.
It should be framed as a research question:
Do inflammatory conditions change hematoma healing patterns?
That is different from saying:
Inflammation is why your hematoma is still there.
The first is responsible.
The second may be overconfident.
Progesterone and immune regulation
Progesterone is central to pregnancy maintenance. It supports the endometrium and decidua, helps maintain uterine quiescence, and has important immunomodulatory roles at the maternal-fetal interface.
Research describes progesterone as influencing immune tolerance, decidual function and inflammatory signaling in pregnancy.
This makes progesterone biologically relevant when discussing pregnancy support.
But relevance is not the same as proof of treatment effect for every hematoma.
Progesterone should not be presented as a universal treatment that prevents or resolves pregnancy hematoma. Its use depends on clinical context, local guidelines, history, symptoms, gestational age and the responsible clinician’s judgment.
A careful statement is:
Progesterone has important roles in pregnancy and immune regulation. In selected clinical contexts, progesterone support may be considered. However, it is not established as a general hematoma-clearing treatment for all patients.
This distinction protects trust.
A proposed model: local vulnerability at the tissue interface
A useful way to think about some pregnancy hematomas is as a local vulnerability event.
The visible hematoma may be the result of several overlapping factors:
- small-vessel bleeding
- membrane or chorionic separation
- placental-edge bleeding
- fragile decidual vessels
- altered implantation biology
- inflammation
- local tissue tension
- clot organization
- limited clearance space
In this model, the hematoma is not just a clot. It is a sign that something happened at a local tissue boundary.
This model is useful for research and education, but it must remain honest.
It is not proven for every case.
It should not be used to blame the patient.
It should not replace clinical assessment.
It should not imply that one supplement, hormone or anti-inflammatory intervention can solve every hematoma.
It is a framework for asking better questions.
What patients often want to know
Many patients with hematoma, especially those with IVF history, endometriosis or previous miscarriage, are already reading deeply.
They do not only want reassurance.
They want coherence.
They may ask:
Could my endometriosis be related?
Could inflammation make bleeding more likely?
Does progesterone calm the tissue?
Why does the hematoma sit near the placenta?
Why is it still there?
Could my immune system affect healing?
Is this an implantation problem?
Is this a placental problem?
What is known, and what is only theory?
These are reasonable questions.
The honest answer is often:
Some of these connections are biologically plausible. Some are supported indirectly by pregnancy outcome research. Some remain unproven. Individual risk cannot be determined from theory alone.
That answer may feel less satisfying than certainty, but it is more scientifically honest.
What can be followed clinically?
If inflammation or tissue-interface vulnerability is suspected as part of the broader context, clinical follow-up still usually depends on concrete findings.
Relevant information may include:
- hematoma location
- size and change over time
- placental relationship
- bleeding pattern
- pain or contractions
- cervix assessment if relevant
- fetal growth
- amniotic fluid
- maternal history
- IVF or miscarriage history
- endometriosis or adenomyosis history
- medication and anticoagulation history
- blood pressure and other pregnancy risk factors
A hypothesis about inflammation is not enough by itself.
It must be connected to observable clinical data.
Why this belongs in Pregnancy Intelligence
Pregnancy hematoma is a good example of why women’s health needs better structured interpretation.
The same finding can be described as:
“a small bleed”
“a subchorionic hematoma”
“a placental-edge collection”
“old blood”
“not concerning”
“something to monitor”
For the patient, these statements may not explain the mechanism or the uncertainty.
Pregnancy Intelligence can help by organizing:
- anatomy
- symptoms
- ultrasound language
- risk context
- biological mechanisms
- evidence level
- open questions
The goal is not to create fear. The goal is to make the uncertainty more structured.
When to seek medical care
Any bleeding during pregnancy should be discussed with a healthcare provider.
Urgent assessment is especially important if there is:
- heavy bleeding
- severe abdominal pain
- dizziness or fainting
- contractions
- fluid leakage
- fever
- uterine tenderness
- reduced fetal movement later in pregnancy
- sudden worsening of symptoms
This article is educational and does not replace clinical care.
Key message
A pregnancy hematoma is a visible blood collection, but the biology around it may involve more than blood alone.
The tissue interface between uterus, decidua, membranes and placenta is vascular, immune-active and biologically complex.
Inflammation, endometriosis, altered decidual function or placental-interface vulnerability may be relevant in some pregnancies, but direct causation is not proven for every case.
The responsible position is to separate what is known, what is plausible and what remains an open research question.
References and Resources
- Subchorionic hematoma: Research status and pathogenesis Medicine International / Spandidos Publications
Background on SCH definition, uncertain pathogenesis, possible mechanisms involving trophoblast invasion, angiogenesis and vascular fragility, and mixed outcome evidence. - Endometriosis and Risk of Adverse Pregnancy Outcome: A Systematic Review and Meta-Analysis Journal of Clinical Medicine / MDPI
Systematic review and meta-analysis reporting associations between endometriosis and several adverse pregnancy outcomes, including preterm birth, placenta previa, placental abruption and hypertensive disorders. - The Effects of Progesterone on Immune Cellular Function at the Maternal-Fetal Interface and Maternal Circulation Journal of Steroid Biochemistry and Molecular Biology / NIH PMC
Review of progesterone’s immunomodulatory roles in decidua, placenta, myometrium and maternal circulation during pregnancy. - Progesterone: A Unique Hormone with Immunomodulatory Roles in Pregnancy International Journal of Molecular Sciences / MDPI
Review describing progesterone’s roles in pregnancy, immune modulation and downregulation of inflammatory reactions. - Bleeding During Pregnancy ACOG — American College of Obstetricians and Gynecologists
Patient safety source supporting that bleeding during pregnancy should be discussed with a healthcare provider.
