
Separating evidence, biology and open research questions
Many women with endometriosis are used to being told that symptoms are “normal,” “stress-related” or “not clearly connected.”
So when a pregnancy hematoma appears during an IVF pregnancy, after previous miscarriage, or in someone with known endometriosis, the question often comes naturally:
Could my endometriosis be related?
The honest answer is nuanced.
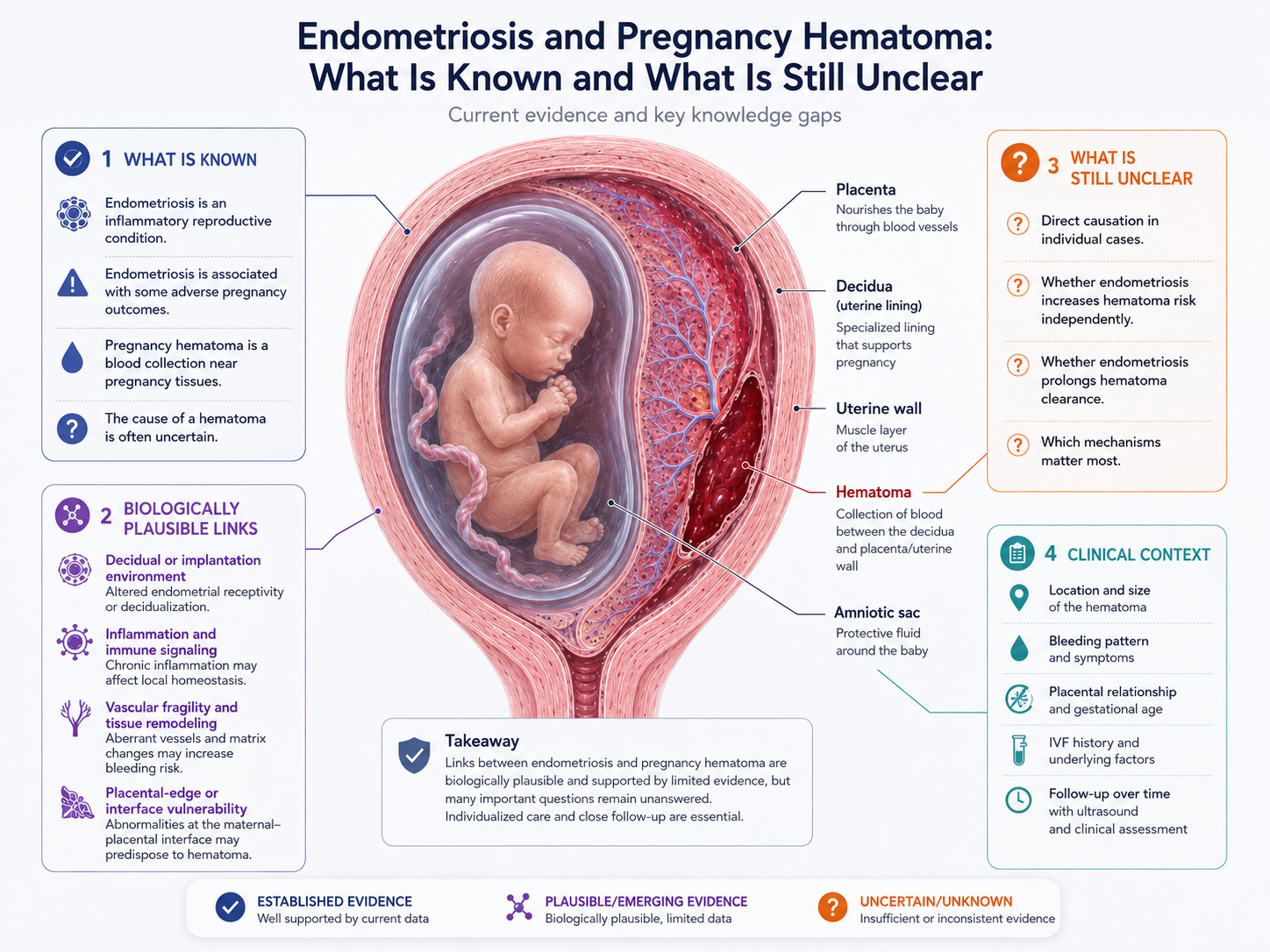
Endometriosis is an inflammatory, hormone-responsive and reproductive condition. It is associated in research with several pregnancy complications, including placental and preterm birth-related outcomes in some studies. However, a direct, proven causal link between endometriosis and pregnancy hematoma is not firmly established for every case.
That distinction matters.
It is reasonable to ask whether endometriosis could contribute to a vulnerable pregnancy tissue interface. But it would be too strong to say that endometriosis is the cause of a specific hematoma without individual evidence.
This article separates what is known, what is biologically plausible and what remains unclear.
What is endometriosis?
Endometriosis is a condition where tissue similar to the endometrium, the lining inside the uterus, exists outside the uterine cavity.
It can affect the ovaries, pelvic peritoneum, bowel, bladder, uterosacral ligaments and other pelvic structures. In some women, it is associated with pain, heavy periods, painful intercourse, bowel or bladder symptoms, fatigue and infertility. In others, symptoms may be mild or atypical.
Endometriosis is not just misplaced tissue.
It is also associated with:
- chronic inflammation
- altered immune signaling
- hormone responsiveness
- pelvic tissue remodeling
- angiogenesis, meaning new blood vessel formation
- fibrosis and adhesions
- altered reproductive environment
This is why endometriosis can be relevant beyond pain alone.
It may influence fertility, implantation biology and pregnancy risk patterns in some women.
What is a pregnancy hematoma?
A pregnancy hematoma is a localized blood collection near pregnancy tissues.
It may be described as:
- subchorionic
- marginal
- subplacental
- retroplacental
- adjacent to the gestational sac
- near the membranes
- near or behind the placenta
Some hematomas are found after vaginal bleeding or spotting. Others are discovered incidentally on ultrasound.
A hematoma is a finding, not a full explanation.
It tells us that blood has collected somewhere, but not always why the bleeding occurred.
That is why the connection to endometriosis is difficult to prove.
What is known: endometriosis is linked to some pregnancy risks
Research has associated endometriosis with several adverse pregnancy outcomes.
Systematic reviews and meta-analyses have reported associations between endometriosis and outcomes such as:
- preterm birth
- placenta previa
- placental abruption
- hypertensive disorders of pregnancy
- cesarean delivery
- stillbirth in some analyses
These associations do not mean that every woman with endometriosis will have complications. Most pregnancies in women with endometriosis do not end in severe adverse outcomes.
But the associations suggest that endometriosis may influence pregnancy biology in some cases.
The important point is this:
Endometriosis appears to be more than a pre-pregnancy pain or fertility condition. It may be connected to placental, inflammatory and vascular aspects of pregnancy.
That makes it reasonable to study its relationship to hematoma formation and persistence.
What is not known: direct causation of pregnancy hematoma
The direct link between endometriosis and pregnancy hematoma is much less clear.
At present, it would be too strong to say:
Endometriosis causes pregnancy hematoma.
A more accurate statement is:
Endometriosis may be part of a biological context that could plausibly influence tissue vulnerability, implantation, placental development or local bleeding risk in some pregnancies, but the direct relationship with pregnancy hematoma remains uncertain.
This distinction is essential for patient trust.
Patients deserve explanations that are serious and coherent, but not overconfident.
Why a connection is biologically plausible
Even though direct proof is limited, several biological ideas make the question reasonable.
Endometriosis may be associated with:
- chronic inflammatory signaling
- altered immune regulation
- changes in angiogenesis
- altered progesterone responsiveness in some contexts
- endometrial or decidual dysfunction
- increased oxidative stress
- altered implantation environment
- higher use of fertility treatment or IVF
A pregnancy hematoma may involve:
- small-vessel bleeding
- local tissue separation
- placental-edge bleeding
- vascular fragility
- decidual or chorionic interface changes
- abnormal or vulnerable placental attachment
- clot organization and healing
These two lists overlap conceptually around inflammation, vessels, implantation and tissue remodeling.
That does not prove causation.
But it does create a plausible research pathway.
The decidual interface: a possible bridge
One of the most interesting concepts is the decidual interface.
During pregnancy, the uterine lining transforms into decidua. The decidua supports implantation, placental development, immune tolerance and vascular remodeling.
If the endometrial environment before pregnancy is altered, it is reasonable to ask whether the decidual environment during pregnancy may also be altered in some women.
In theory, this could affect:
- how the placenta attaches
- how maternal vessels remodel
- how local inflammation is controlled
- how tissue responds to bleeding
- how stable the membrane-uterine interface becomes
This is not a proven explanation for every hematoma. But it is a coherent biological hypothesis.
For women with endometriosis, adenomyosis, IVF history or repeated pregnancy complications, this tissue-interface model may be especially relevant as an applied research question.
IVF makes interpretation more complicated
Many women with endometriosis conceive through IVF.
This creates a common interpretive problem.
If a hematoma is found in an IVF pregnancy, what is responsible?
Possible contributors could include:
- endometriosis biology
- underlying infertility factors
- embryo transfer and implantation context
- hormonal preparation
- maternal age
- uterine factors
- closer early ultrasound surveillance
- chance
IVF pregnancies are scanned more frequently, especially early. This may increase detection of hematomas that might otherwise have gone unnoticed.
So the presence of hematoma after IVF does not automatically mean IVF caused it, and it does not automatically mean endometriosis caused it.
The correct interpretation is usually broader:
A hematoma in an IVF pregnancy may reflect a combination of pregnancy biology, patient background, monitoring intensity and local tissue factors.
Could endometriosis affect hematoma persistence?
Formation and persistence are not necessarily the same question.
A hematoma may form because of a local bleeding event. It may persist because blood is trapped, organized, slowly resorbed, or only partially drained.
Could endometriosis influence persistence?
Possibly, but this remains uncertain.
A theoretical link could involve:
- altered inflammatory healing
- local immune activation
- vascular remodeling differences
- tissue fragility
- slower resolution of blood products
- persistence of irritation at the decidual interface
But these are research hypotheses. They should not be presented as established clinical facts.
The safer formulation is:
Endometriosis may be relevant to the broader inflammatory and reproductive context, but whether it directly affects hematoma resolution time is not well established.
What patients often experience
Patients with endometriosis often have a history of not being fully heard.
They may have spent years connecting symptoms that were dismissed as unrelated. They may have needed to fight for diagnosis. They may have undergone fertility treatment, surgery or repeated investigations.
So when pregnancy bleeding or hematoma occurs, they may not be satisfied with a simple answer like:
“It just happens.”
That answer may be true in some cases, but it may also feel incomplete.
A more respectful answer is:
A hematoma can occur in many pregnancies and often no single cause is identified. In women with endometriosis, it is reasonable to consider the broader inflammatory, vascular and implantation context, but current evidence does not prove that endometriosis directly caused the hematoma in every case.
This gives both validation and scientific caution.
What can be followed clinically?
Even if endometriosis is part of the background, clinical follow-up usually depends on observable pregnancy findings.
Important factors may include:
- hematoma location
- hematoma size
- change over time
- relationship to placenta
- bleeding pattern
- pain or contractions
- cervical findings if relevant
- placental position
- fetal growth
- IVF or miscarriage history
- endometriosis or adenomyosis history
- medication history
- maternal blood pressure and other risk factors
A theory about endometriosis does not replace pregnancy monitoring.
It may help frame questions, but the clinical picture still matters most.
What would better research need?
To understand the relationship between endometriosis and pregnancy hematoma, better studies would need to separate several factors.
Useful research questions include:
Do women with endometriosis have higher rates of pregnancy hematoma after adjusting for IVF, age and other factors?
Are hematomas in endometriosis pregnancies more likely to be marginal, subchorionic or retroplacental?
Does endometriosis severity matter?
Does adenomyosis change the risk pattern?
Are hematomas more persistent in women with inflammatory reproductive history?
Do progesterone response, immune markers or vascular markers correlate with hematoma formation?
Can ultrasound features identify different biological subtypes of hematoma?
Can symptom tracking improve interpretation between scans?
These are not settled questions.
But they are exactly the kind of questions women’s health research should ask.
Avoiding blame
This topic must be handled carefully.
If a woman has endometriosis and develops a pregnancy hematoma, she should not be made to feel that her body failed or that she caused the complication.
Endometriosis is a medical condition. Pregnancy hematoma can occur for many reasons. In many cases, the exact cause is unknown.
The goal of discussing endometriosis is not blame.
The goal is better understanding, better research questions and more respectful interpretation of complex pregnancy histories.
When to seek medical care
Any bleeding during pregnancy should be discussed with a healthcare provider.
Urgent assessment is especially important if there is:
- heavy bleeding
- severe abdominal pain
- dizziness or fainting
- contractions
- fluid leakage
- fever
- uterine tenderness
- reduced fetal movement later in pregnancy
- sudden worsening of symptoms
This article is educational and does not replace clinical care.
Key message
Endometriosis may be relevant to pregnancy hematoma as part of a broader inflammatory, vascular and implantation context.
But a direct causal link is not proven for every case.
The honest position is this:
Endometriosis is associated with altered reproductive biology and some adverse pregnancy outcomes. Pregnancy hematoma is a blood collection near pregnancy tissues with often uncertain cause. A connection between the two is biologically plausible in some cases, but remains an open research question.
Good women’s health intelligence should be able to hold both truths at the same time.
References and Resources
- Endometriosis and Risk of Adverse Pregnancy Outcome: A Systematic Review and Meta-Analysis Journal of Clinical Medicine / MDPI
This systematic review reports associations between endometriosis and several adverse pregnancy outcomes, including preterm birth, placenta previa, placental abruption, hypertensive disorders, cesarean delivery and stillbirth. - Endometriosis Guideline ESHRE — European Society of Human Reproduction and Embryology
ESHRE guideline for diagnosis and management of endometriosis, including pain, infertility and medically assisted reproduction. - ESHRE Guideline: Endometriosis Human Reproduction Open / Oxford Academic
Published summary of the ESHRE endometriosis guideline with evidence-based recommendations - Subchorionic hematoma: Research status and pathogenesis Medicine International / Spandidos Publications
Review describing SCH definition, unclear etiology/pathogenesis, possible mechanisms and controversial outcome evidence - Bleeding During Pregnancy ACOG — American College of Obstetricians and Gynecologists
Patient safety source stating that bleeding during pregnancy should be discussed with an obstetric provider.
