
A structured overview of what endometriosis is, how it behaves and what may reduce its impact
Endometriosis is often described as a condition where tissue similar to the uterine lining grows outside the uterus.
That description is true, but incomplete.
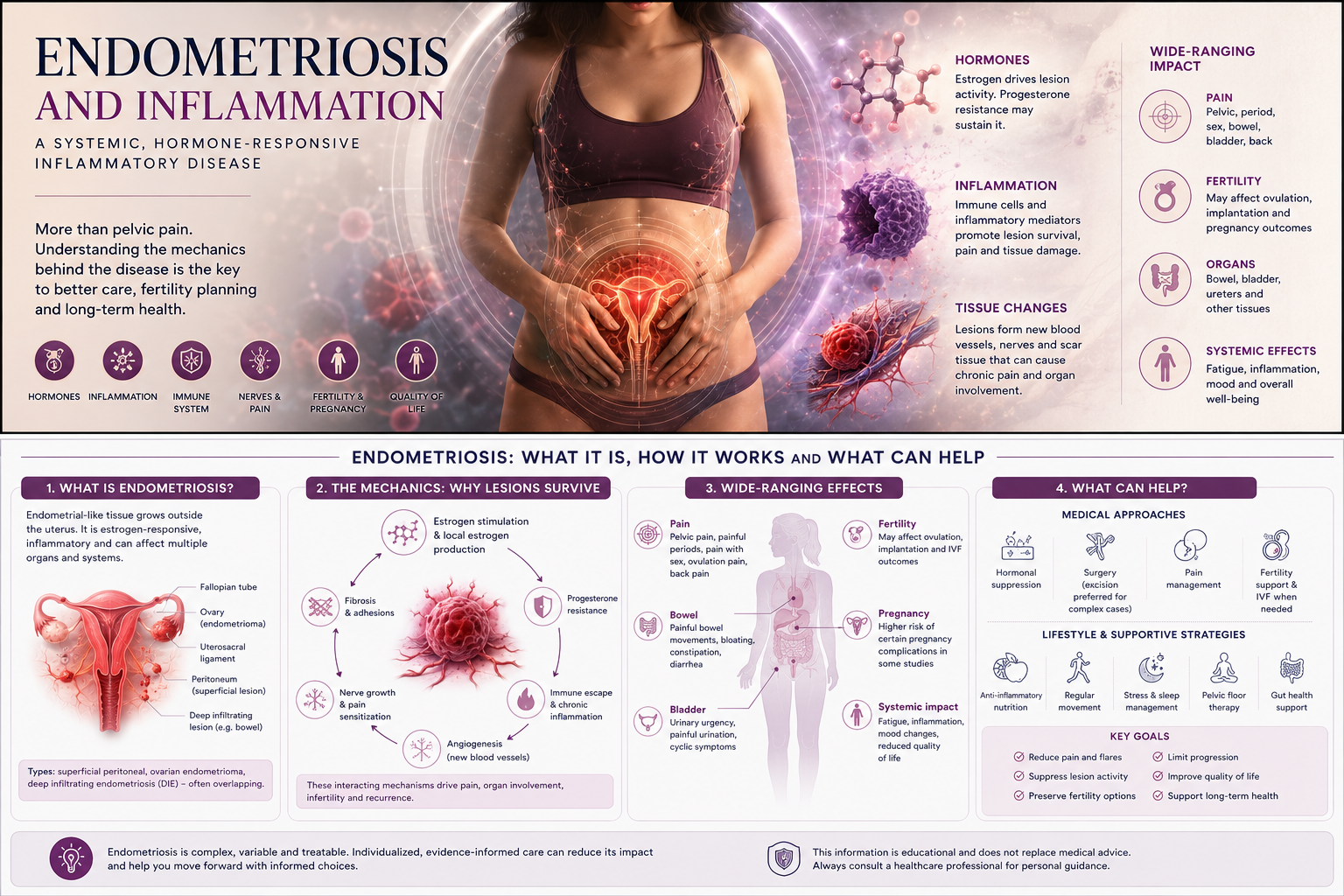
Endometriosis is not only “misplaced tissue.” It is a chronic, estrogen-responsive, inflammatory and tissue-remodeling disease that can affect pain, fertility, bowel function, bladder symptoms, fatigue, immune signaling, pregnancy biology and long-term quality of life.
For many women, the problem is not only the disease itself. It is the lack of coherent explanation.
Pain may be dismissed. Bowel symptoms may be separated from gynecology. Fertility issues may be treated as a different problem. Inflammation may be mentioned but not explained. Hormone treatment may be offered without a clear model of what it is trying to control.
This article gives a structured overview of endometriosis as a biological system:
What is it?
How does it start?
How do lesions survive?
Why does it cause pain?
Why can it affect fertility?
What role does inflammation play?
What can be done to reduce symptoms, suppress activity or limit its impact?
The goal is not to oversimplify endometriosis.
The goal is to make the mechanics understandable.
What exactly is endometriosis?
Endometriosis is a condition where tissue that resembles the endometrium, the lining inside the uterus, is found outside the uterine cavity.
This endometrial-like tissue may appear on or within:
- the pelvic peritoneum
- ovaries
- fallopian tubes
- uterosacral ligaments
- bowel surface or bowel wall
- bladder or urinary tract
- rectovaginal septum
- pelvic nerves or deeper pelvic tissue
- surgical scars in rare cases
- distant locations in rare cases
Endometriosis lesions are not identical to normal uterine lining. They behave differently. They may be hormonally active, inflammatory, invasive, fibrotic, vascularized and neurologically sensitive.
Endometriosis is commonly grouped into different forms:
Superficial peritoneal endometriosis
Lesions are found on the peritoneal surface, the thin lining inside the pelvis. These lesions may look small, but size does not always predict pain.
Ovarian endometrioma
This is an endometriosis-related ovarian cyst, often called a “chocolate cyst” because it contains old blood products.
Deep endometriosis
Lesions grow deeper into tissues, often involving structures such as the uterosacral ligaments, bowel, bladder or rectovaginal area. Deep endometriosis can cause severe pain and organ-specific symptoms.
These types can overlap. A woman may have one form or several.
Why endometriosis is not just “period pain”
Painful periods are common in endometriosis, but endometriosis pain is often more complex.
Symptoms may include:
- severe menstrual pain
- pelvic pain outside menstruation
- pain during or after sex
- bowel pain
- painful bowel movements
- bloating or IBS-like symptoms
- bladder pain or urinary symptoms
- ovulation pain
- lower back or leg pain
- fatigue
- infertility
- pain after gynecological procedures
- pain that continues despite normal imaging
The symptom pattern depends on lesion location, nerve involvement, inflammation, adhesions, hormonal response and pain sensitization.
A woman can have severe symptoms with small lesions. Another woman can have extensive disease and relatively little pain.
This mismatch is one reason endometriosis is often misunderstood.
How might endometriosis start?
There is no single theory that explains all endometriosis.
Several mechanisms may contribute, and different mechanisms may matter in different patients.
Retrograde menstruation
One classic theory is that menstrual blood flows backward through the fallopian tubes into the pelvis. This may carry endometrial cells into the pelvic cavity.
However, retrograde menstruation is common, while endometriosis affects only some women. So retrograde menstruation alone is not enough.
Other factors must influence whether those cells survive, attach and grow.
Immune escape
Normally, misplaced cells should be cleared by immune surveillance. In endometriosis, immune clearance may be altered.
Cells may survive in the wrong place because the local immune environment allows them to persist.
Coelomic metaplasia
Another theory is that certain cells in the pelvic lining can transform into endometrial-like cells under specific biological signals.
This may help explain endometriosis in unusual locations or cases not easily explained by retrograde menstruation.
Stem or progenitor cells
Some researchers have proposed that stem-like cells from the endometrium or bone marrow may contribute to lesion formation.
Lymphatic or vascular spread
In rare or distant endometriosis, cells may spread through blood or lymphatic pathways.
The important point is this:
Endometriosis probably does not have one single origin.
It is better understood as a disease where misplaced or transformed endometrial-like tissue survives in an environment that allows inflammation, vascular growth, nerve interaction and fibrosis.
The mechanics of endometriosis: how lesions survive
Once endometrial-like cells are outside the uterus, they must overcome several barriers to become endometriosis lesions.
They need to:
- survive outside their normal location
- attach to tissue
- avoid immune clearance
- create a blood supply
- respond to hormones
- produce inflammatory signals
- remodel surrounding tissue
- interact with nerves
- persist over time
This is why endometriosis behaves less like a passive implant and more like an active tissue system.
Mechanic 1: Hormone dependence
Endometriosis is strongly influenced by estrogen.
Estrogen can support lesion survival, inflammation and growth. Some endometriosis lesions can also produce local estrogen through increased aromatase activity.
This creates a local hormonal environment that may help sustain the disease.
Progesterone normally counterbalances some estrogen-driven effects in the endometrium. But in endometriosis, progesterone responsiveness may be impaired in some tissues. This is often described as progesterone resistance.
This matters because many treatments aim to reduce estrogen stimulation or increase progestogenic suppression.
Mechanic 2: Progesterone resistance
Progesterone resistance means that tissue does not respond normally to progesterone signaling.
In endometriosis, this may contribute to:
- persistent inflammation
- impaired decidualization
- altered endometrial receptivity
- abnormal immune signaling
- reduced suppression of estrogen-driven activity
- fertility-related problems in some women
Progesterone resistance does not mean progesterone is irrelevant. It means the response may be altered.
This may help explain why some patients respond well to progestin-based treatment while others do not.
It may also connect endometriosis to fertility and implantation research.
Mechanic 3: Inflammation
Inflammation is central to endometriosis.
Endometriosis lesions and the surrounding pelvic environment may contain activated immune cells and inflammatory mediators. Macrophages, mast cells, cytokines, prostaglandins, oxidative stress and immune signaling pathways may all contribute.
Inflammation may help explain:
- pain
- tissue irritation
- fatigue
- lesion survival
- angiogenesis
- adhesions
- altered fertility environment
- bowel and bladder sensitivity
- flare patterns
Inflammation is not just a side effect.
It is part of the disease machinery.
Mechanic 4: Angiogenesis
Endometriosis lesions need blood supply to survive.
Angiogenesis means formation of new blood vessels. Lesions may stimulate local blood vessel growth to obtain oxygen and nutrients.
This is one reason endometriosis can persist and recur.
It is also why endometriosis is not just a surface stain. It can become biologically integrated into surrounding tissue.
Mechanic 5: Nerve growth and pain signaling
Endometriosis can interact with nerves.
Lesions may contain or attract nerve fibers. Inflammatory mediators can sensitize nerves and lower the threshold for pain.
Over time, pain can become amplified through peripheral and central sensitization.
This means the nervous system may become more reactive even if lesion size does not fully explain symptoms.
Pain in endometriosis can therefore involve:
- local tissue inflammation
- nerve invasion or nerve proximity
- pelvic floor muscle guarding
- bowel or bladder sensitization
- central pain processing
- repeated inflammatory flares
This is why treating endometriosis pain may require more than removing visible lesions.
Mechanic 6: Fibrosis and adhesions
Inflammation and tissue repair can lead to fibrosis.
Fibrosis means scar-like tissue remodeling. Adhesions are bands of tissue that can bind organs or surfaces together.
In endometriosis, fibrosis and adhesions can distort pelvic anatomy.
This may contribute to:
- pain
- reduced organ mobility
- bowel symptoms
- infertility
- surgical complexity
- recurrent symptoms
- chronic pelvic tension
Deep endometriosis is especially associated with fibrotic tissue remodeling.
This is one reason early recognition matters.
Mechanic 7: Organ-specific effects
Endometriosis symptoms often depend on where lesions are located.
Ovaries
Endometriomas may affect ovarian reserve, inflammation and fertility planning.
Bowel
Bowel involvement may cause pain with bowel movements, diarrhea, constipation, bloating, cyclic rectal pain or deep pelvic pain.
Bladder
Bladder involvement may cause urinary urgency, bladder pain, pain with filling or cyclic urinary symptoms.
Uterosacral ligaments and pelvic nerves
These locations may cause deep pelvic pain, pain during sex, lower back pain or radiating leg pain.
This is why endometriosis should not be understood only as a uterine condition.
It is a pelvic and sometimes systemic disease.
Endometriosis and fertility
Endometriosis can affect fertility through several possible mechanisms.
These may include:
- distorted pelvic anatomy
- adhesions affecting tubes or ovaries
- endometriomas affecting ovarian reserve
- inflammation in the pelvic environment
- altered egg quality in some cases
- altered sperm-egg interaction
- impaired implantation environment
- progesterone resistance
- changes in endometrial receptivity
In some women, surgery improves fertility chances. In others, IVF may be needed. In some cases, fertility is preserved despite endometriosis.
The key point is that fertility impact varies.
Endometriosis should be assessed individually, not assumed to have the same effect in every woman.
Endometriosis and pregnancy biology
Endometriosis is often discussed mainly before pregnancy, but it may also be relevant during pregnancy.
Research has associated endometriosis with increased risk of certain pregnancy complications in some studies, including preterm birth, placenta previa, placental abruption and hypertensive disorders.
The mechanisms are not fully understood.
Possible links may involve:
- altered implantation
- decidualization differences
- placental development
- inflammation
- vascular remodeling
- adenomyosis overlap
- IVF and infertility factors
This does not mean that every pregnancy with endometriosis is high risk.
It means endometriosis may carry information about the reproductive environment.
That makes it important in Pregnancy Intelligence.
Can endometriosis be slowed down?
There is no simple cure for endometriosis.
But its activity, symptoms and consequences can often be reduced.
The realistic goals may include:
- reduce pain
- suppress cyclic lesion stimulation
- reduce inflammatory flares
- preserve fertility options
- limit progression where possible
- treat deep disease or organ involvement
- improve quality of life
- reduce recurrence risk after surgery
- support long-term monitoring
Treatment depends on symptoms, age, fertility goals, lesion type, severity, prior surgery, medication tolerance and personal priorities.
Medical strategies to reduce activity and symptoms
Hormonal suppression
Hormonal treatment is often used to reduce estrogen-driven cycling and suppress lesion activity.
Options may include:
- combined hormonal contraceptives
- progestins
- levonorgestrel intrauterine system
- GnRH agonists
- GnRH antagonists
- add-back therapy when needed
- other specialist-directed hormonal strategies
These treatments do not remove endometriosis lesions, but they may reduce stimulation, bleeding-like activity, inflammation and pain in many patients.
They are often used when pregnancy is not currently being attempted.
Surgery
Surgery may be used to diagnose and treat endometriosis, especially when symptoms are severe, deep disease is suspected, organs are involved, fertility is affected, or medical treatment is insufficient.
Surgery may include excision or ablation, but excision by experienced surgeons is often emphasized for deep or complex disease.
Surgery is not automatically curative. Recurrence can occur, and pain may persist if there is nerve sensitization, pelvic floor dysfunction or remaining disease.
Pain management
Pain management may include anti-inflammatory medication, hormonal suppression, nerve pain strategies, pelvic floor physiotherapy, multidisciplinary pain care and treatment of overlapping bowel or bladder conditions.
Endometriosis pain is often multi-layered. The best care may need to address lesions, inflammation, nerves, muscles and central pain sensitivity.
Lifestyle and supportive strategies: what may help
Lifestyle cannot cure endometriosis, and women should not be blamed for the disease.
But supportive strategies may reduce symptom burden and inflammatory load in some individuals.
Potentially helpful areas include:
Anti-inflammatory dietary pattern
Some women report symptom improvement with dietary changes. Research is still developing and not all studies are strong, but anti-inflammatory patterns, omega-3 intake, adequate fiber and attention to gut triggers may help some patients.
This should be individualized.
Gut health and IBS overlap
Many women with endometriosis have bowel symptoms or IBS-like patterns. Identifying food triggers, treating constipation, managing bloating and addressing gut inflammation may reduce overall symptom load.
Physical activity
Regular movement may support inflammation regulation, mood, sleep, insulin sensitivity and pain modulation. Exercise should be adapted to pain level and fatigue.
Sleep and stress physiology
Poor sleep and chronic stress can amplify pain sensitivity and inflammatory signaling. Sleep support and nervous system regulation may improve resilience, even if they do not remove lesions.
Pelvic floor therapy
Pelvic floor muscles often become tense and protective in chronic pelvic pain. Pelvic floor physiotherapy can be important when pain continues despite hormonal or surgical treatment.
Nutrient status
Vitamin D, iron status, omega-3 intake, magnesium and other nutrients may be relevant in selected patients, especially with heavy bleeding, fatigue, dietary restriction or inflammation. Testing and individualized interpretation are preferable to random supplementation.
The responsible message is:
Lifestyle and supportive care may reduce impact, but they are not substitutes for appropriate medical assessment and treatment.
What not to overpromise
Endometriosis care is full of overclaims.
It is important not to say:
Diet cures endometriosis.
Supplements remove lesions.
Pregnancy cures endometriosis.
Menopause always ends endometriosis.
Surgery always cures pain.
Hormones work for everyone.
Normal ultrasound excludes endometriosis.
Pain level always matches disease severity.
These claims are too simplistic.
A serious women’s health platform should be more precise.
What can be monitored?
Endometriosis monitoring may include:
- symptom pattern
- pain timing
- bleeding pattern
- bowel and bladder symptoms
- fertility goals
- imaging when relevant
- ovarian reserve markers when fertility is relevant
- anemia or iron status
- inflammation-related markers in selected contexts
- medication response
- recurrence after surgery
- quality of life
- pregnancy outcomes
- long-term hormonal transition
There is no single blood test that reliably diagnoses endometriosis in routine care.
That makes structured symptom history and specialist assessment very important.
A systems model of endometriosis
Endometriosis can be understood as a system involving:
Hormones
↓
Immune signaling
↓
Inflammation
↓
Lesion survival
↓
Blood vessel growth
↓
Nerve sensitization
↓
Fibrosis and adhesions
↓
Pain, fertility effects and organ symptoms
This does not mean every patient has every mechanism.
But it helps explain why endometriosis can be so persistent and variable.
Why this category matters
Endometriosis sits at the intersection of several High Coast Women’s Health Intelligence areas:
- hormone health
- fertility and IVF
- pregnancy intelligence
- inflammation
- menopause and postmenopause
- women’s longevity
- biomarker interpretation
- pain and quality of life
It is one of the best examples of why women’s health needs a more integrated model.
The disease is biological.
The symptoms are real.
The mechanisms are complex.
The care must be individualized.
The uncertainty should be explained, not hidden.
Key message
Endometriosis is more than pelvic pain.
It is a chronic inflammatory, hormone-responsive and tissue-remodeling condition that can affect pain, fertility, pregnancy biology and long-term health.
The mechanics include hormone dependence, progesterone resistance, inflammation, angiogenesis, nerve sensitization, fibrosis and organ-specific involvement.
There is no single cure, but many strategies can reduce its impact.
The strongest approach is usually structured, individualized and long-term: accurate diagnosis, symptom mapping, hormonal or surgical treatment when appropriate, fertility planning, inflammation-aware support, pain management and follow-up over time.
References
Endometriosis guideline ESHRE — European Society of Human Reproduction and Embryology
Best-practice guideline covering diagnosis, pain treatment, infertility and medically assisted reproduction in endometriosis.
Endometriosis: diagnosis and management NICE — National Institute for Health and Care Excellence
Guideline covering diagnosis and management of endometriosis, including symptom awareness, referral, diagnosis and treatment options
ESHRE guideline: endometriosis Human Reproduction Open / Oxford Academic
Published evidence-based summary of the ESHRE guideline, including classification into peritoneal endometriosis, deep endometriosis and endometrioma
Endometriosis and the Role of Pro-Inflammatory and Anti-Inflammatory Cytokines in Pathophysiology NIH PMC
Review of inflammatory mechanisms in endometriosis, including immune cells, cytokines, oxidative stress, estrogen synthesis and progesterone resistance
Endometriosis and the effects of dietary interventions: what are we looking for? NIH PMC
Review discussing dietary interventions and the uncertainty around which interventions are most effective and why
Effect of Dietary Interventions on Endometriosis: A Systematic Review and Meta-Analysis Reproductive Sciences / Springer
Systematic review noting possible symptom effects but highlighting heterogeneity, risk of bias and need for more randomized trials.
