
Understanding pregnancy risk without creating unnecessary fear
Endometriosis is often discussed before pregnancy: pain, fertility, IVF, surgery, ovarian reserve and implantation.
But many women also ask what endometriosis means after pregnancy has already started.
Does endometriosis increase pregnancy risk?
Does it affect the placenta?
Does it increase miscarriage risk?
Does it make bleeding more likely?
Does it matter if conception happened through IVF?
Should pregnancy monitoring be different?
These are important questions.
The answer is not that every pregnancy with endometriosis is dangerous. Many women with endometriosis have healthy pregnancies and healthy babies.
But research suggests that endometriosis may be associated with increased risk of certain pregnancy complications in some groups. The pattern is not always simple, and risk can depend on disease type, severity, adenomyosis, IVF history, maternal age, previous surgery and other factors.
This article gives a structured overview of what is known, what is biologically plausible and what remains uncertain.
Why endometriosis can matter during pregnancy
Endometriosis is not only a pain condition.
It is a chronic inflammatory, hormone-responsive and tissue-remodeling condition. It can affect the pelvis, ovaries, bowel, bladder, immune signaling, angiogenesis, fibrosis and fertility.
Pregnancy does not erase that biological history.
When pregnancy begins, the uterus, decidua, placenta and maternal immune system must coordinate a complex process:
- implantation
- decidualization
- placental development
- vascular remodeling
- immune tolerance
- fetal growth
- uterine expansion
- long-term pregnancy maintenance
Endometriosis may be relevant because it is linked to inflammation, altered reproductive biology and, in some women, altered implantation or placental-interface function.
This does not mean endometriosis directly causes every pregnancy problem.
It means endometriosis may be part of the pregnancy risk context.
What pregnancy outcomes have been associated with endometriosis?
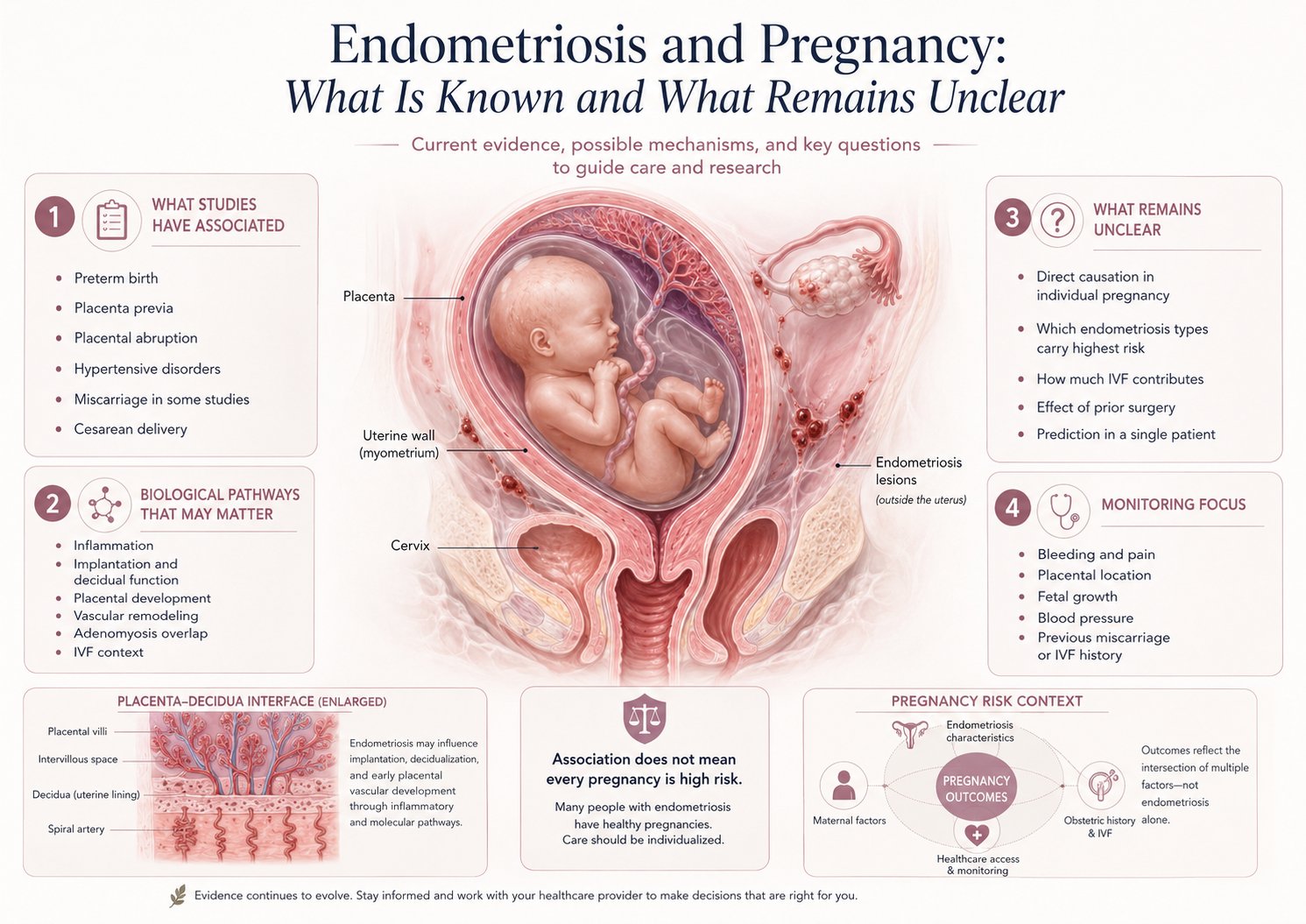
Several systematic reviews and meta-analyses have reported associations between endometriosis and certain adverse pregnancy outcomes.
These may include:
- preterm birth
- placenta previa
- placental abruption
- hypertensive disorders of pregnancy
- cesarean delivery
- miscarriage in some studies
- small-for-gestational-age infant in some analyses
- stillbirth in some analyses
This does not mean every woman with endometriosis has a high-risk pregnancy.
It means that, at population level, women with endometriosis may have higher rates of some complications compared with women without endometriosis.
The key word is association.
Association does not always prove direct causation. Some of the increased risk may be related to endometriosis itself. Some may be related to infertility, IVF, adenomyosis, prior surgery, maternal age or other factors.
Why the placenta is central
Many of the pregnancy complications linked to endometriosis involve the placenta or placental environment.
Examples include:
- placenta previa
- placental abruption
- fetal growth restriction
- preterm birth
- hypertensive disorders
This suggests that the implantation and placental-development phase may be important.
The placenta is not just a passive organ. It must attach to the uterine wall, connect with maternal blood flow and support fetal growth.
For this to work well, the pregnancy tissue interface must regulate:
- maternal immune tolerance
- blood vessel remodeling
- inflammation
- oxygen and nutrient exchange
- local tissue stability
- hormonal signaling
Endometriosis may be relevant because it is associated with inflammatory and reproductive changes that could, in some women, influence this interface.
But this remains a complex research area.
Endometriosis, decidua and implantation biology
During pregnancy, the uterine lining becomes decidua.
The decidua is the specialized pregnancy lining that supports implantation, early placental development, immune tolerance and maternal-fetal communication.
In endometriosis, research has described altered inflammatory signaling, progesterone response, immune regulation and endometrial function.
This raises a biologically plausible question:
Could altered endometrial or decidual function contribute to some pregnancy risks in women with endometriosis?
The answer is probably yes in some cases, but not always, and not in a way that can be easily measured in routine care.
This is why individualized pregnancy risk assessment is difficult.
A woman may have endometriosis, but we may not know whether her decidual or placental interface is meaningfully affected.
Adenomyosis: an important overlapping condition
Adenomyosis is a related but different condition where endometrial-like tissue is found within the muscular wall of the uterus.
It can coexist with endometriosis.
This matters because adenomyosis may affect the uterus more directly than pelvic endometriosis alone. It may be linked to implantation problems, miscarriage, preterm birth and other pregnancy complications in some studies.
When a woman with endometriosis has pregnancy concerns, adenomyosis should sometimes be considered, especially if there is a history of heavy periods, enlarged uterus, uterine pain, infertility or recurrent pregnancy loss.
Endometriosis and adenomyosis are not the same condition, but they can overlap and may shape pregnancy risk together.
IVF pregnancies: why interpretation is more complicated
Many women with endometriosis conceive through IVF.
This creates an important interpretation challenge.
If a pregnancy complication occurs after IVF, what is responsible?
Possible contributors may include:
- endometriosis biology
- adenomyosis
- infertility factors
- maternal age
- ovarian reserve
- embryo transfer context
- hormone preparation
- frozen versus fresh transfer
- multiple pregnancy if relevant
- closer early pregnancy surveillance
- background medical factors
IVF can help overcome some barriers to conception, but it does not remove every underlying biological factor.
At the same time, IVF pregnancies are monitored more closely. This means some findings may be detected more often simply because more scans and tests are performed.
So the correct interpretation is careful:
An IVF pregnancy in a woman with endometriosis may need structured monitoring, but a complication should not automatically be blamed on IVF or endometriosis alone.
Does pregnancy “cure” endometriosis?
No.
Pregnancy may suppress menstruation and change hormone patterns, so some women experience symptom relief during pregnancy. But pregnancy does not remove endometriosis lesions.
After pregnancy, symptoms may return, especially after cycles resume.
Some women improve for a period. Others have persistent or recurrent symptoms. Some may have pain related to adhesions, deep disease, bowel or bladder involvement, or pelvic floor changes.
It is more accurate to say:
Pregnancy may temporarily reduce endometriosis activity or symptoms in some women, but it is not a cure.
Does endometriosis increase miscarriage risk?
The evidence is mixed.
Some studies have reported higher miscarriage risk in women with endometriosis, while others show more complex patterns depending on population, disease type, infertility, IVF, age and study design.
Miscarriage is multifactorial. Chromosomal factors, uterine factors, immune factors, endocrine factors, age, embryo quality and chance can all matter.
Endometriosis may be one part of the risk context, especially through inflammation, implantation biology, progesterone response or adenomyosis overlap, but it should not be presented as the cause of every miscarriage in women with endometriosis.
The responsible position is:
Endometriosis may be associated with miscarriage risk in some studies, but individual risk depends on several factors and should be interpreted clinically.
Does endometriosis increase bleeding or hematoma risk?
This is an important question, but the answer is not fully established.
Endometriosis has been associated with placental and pregnancy complications in some research. It is also biologically plausible that inflammation, altered decidual function or vascular remodeling could contribute to bleeding vulnerability in some pregnancies.
However, a direct causal link between endometriosis and pregnancy hematoma is not firmly proven for every case.
A careful statement is:
Endometriosis may be relevant to the biological context of implantation, decidua and placenta. It may be worth considering in women with hematoma, bleeding, IVF history or previous pregnancy loss. But current evidence does not prove that endometriosis directly causes pregnancy hematoma in all cases.
That is the right balance between validation and scientific honesty.
What pregnancy monitoring may focus on
Pregnancy monitoring in women with endometriosis should be individualized.
Depending on history and clinical findings, clinicians may pay attention to:
- early pregnancy location and viability
- bleeding episodes
- pain pattern
- placental location
- fetal growth
- cervical length when relevant
- signs of preterm birth risk
- blood pressure
- symptoms of placental complications
- adenomyosis or uterine factors
- IVF-related pregnancy context
- previous miscarriage or preterm birth history
Not every woman with endometriosis needs intensive monitoring. But some may benefit from more structured follow-up, especially if there are additional risk factors.
Why symptoms can be difficult to interpret during pregnancy
Endometriosis symptoms and normal pregnancy symptoms can overlap.
Pelvic pressure, stretching pain, bowel changes, bladder symptoms and lower abdominal discomfort may occur in normal pregnancy. But women with endometriosis may also have adhesions, deep lesions, bowel involvement or chronic pelvic pain sensitivity.
This can make interpretation difficult.
A woman with known endometriosis may need clearer guidance on which symptoms are expected and which should prompt contact with care.
Symptoms that deserve clinical attention include:
- heavy bleeding
- severe or persistent pain
- contractions
- fever
- fainting or dizziness
- fluid leakage
- significant bowel or bladder pain
- reduced fetal movement later in pregnancy
- sudden worsening of symptoms
The point is not to create fear.
The point is to avoid dismissing symptoms automatically.
What can be done during pregnancy?
During pregnancy, endometriosis treatment options are different from before pregnancy.
Hormonal suppression, many pain medications and elective surgeries are usually not handled the same way during pregnancy.
The focus often shifts toward:
- obstetric monitoring
- symptom evaluation
- safe pain management when needed
- assessment of bleeding or acute pain
- placental and fetal follow-up if indicated
- individualized risk assessment
- postpartum planning
Some women need very little extra care. Others need closer follow-up because of previous miscarriage, IVF, deep disease, adenomyosis, bleeding, placenta-related concerns or preterm birth risk.
The most important principle is individualized care.
Postpartum: the story is not over
After delivery, endometriosis may become relevant again.
Important postpartum questions include:
- When do symptoms return?
- Does breastfeeding delay menstrual cycling and symptoms?
- Is hormonal suppression appropriate after pregnancy?
- Is fertility desired again soon?
- Is there persistent pelvic pain?
- Are bowel, bladder or pelvic floor symptoms present?
- Should surgery be reconsidered later?
- Should long-term disease control be planned?
Pregnancy should not be treated as the end of the endometriosis story.
For many women, postpartum planning is an important part of long-term care.
What remains unclear
Many questions remain open.
Does endometriosis itself drive pregnancy risk, or is risk mainly explained by infertility, IVF, adenomyosis or other factors?
Do different types of endometriosis have different pregnancy risk patterns?
Does deep endometriosis carry different risks than superficial disease?
Does surgical treatment before pregnancy reduce or increase certain risks?
How does adenomyosis change the picture?
Can inflammation markers predict complications?
Can better early pregnancy monitoring identify risk patterns sooner?
Should pregnancy care pathways differ for women with endometriosis?
These questions are not fully settled.
That is why this topic belongs in Evidence Insights and Pregnancy Intelligence.
Key message
Endometriosis can matter during pregnancy, but it does not define the pregnancy.
Many women with endometriosis have healthy pregnancies.
At the same time, research suggests that endometriosis may be associated with certain pregnancy complications, especially those involving placental location, placental function, preterm birth and hypertensive disorders.
The most responsible approach is not fear and not dismissal.
It is structured interpretation:
What type of endometriosis?
Was IVF involved?
Is adenomyosis present?
Is there bleeding or pain?
Where is the placenta?
Is fetal growth reassuring?
What is the previous pregnancy history?
What follow-up is appropriate?
Good pregnancy care should recognize endometriosis as a relevant context without turning it into a prediction.
References and Resource
- Endometriosis guideline ESHRE — European Society of Human Reproduction and Embryology
Best-practice guidance on diagnosis, pain treatment, infertility, assisted reproduction, pregnancy-related information and long-term care in endometriosis. - Endometriosis: diagnosis and management NICE — National Institute for Health and Care Excellence
Guideline covering diagnosis and management of endometriosis, including fertility-priority care and referral to specialist services - ESHRE guideline: endometriosis Human Reproduction Open / Oxford Academic
Published summary of the ESHRE guideline, including endometriosis types, diagnosis, treatment, infertility and broader care topics - Endometriosis and Risk of Adverse Pregnancy Outcome: A Systematic Review and Meta-Analysis Journal of Clinical Medicine / MDPI
Systematic review and meta-analysis reporting associations between endometriosis and several adverse pregnancy outcomes - Endometriosis and obstetrics complications: a systematic review and meta-analysis Fertility and Sterility
Meta-analysis reporting associations between diagnosed endometriosis and poorer pregnancy outcomes, including preterm birth, miscarriage, placenta previa, SGA and cesarean delivery
