
Understanding one of the most important mechanisms behind inflammation, fertility problems and treatment response
Progesterone is one of the key hormones in women’s reproductive health.
It helps regulate the menstrual cycle, prepares the uterine lining for implantation, supports early pregnancy and normally counterbalances some estrogen-driven effects in the endometrium.
So when we talk about endometriosis, progesterone should be central.
But in endometriosis, the problem is not only how much progesterone is present.
The deeper question is:
Does the tissue respond normally to progesterone?
This is where the concept of progesterone resistance becomes important.
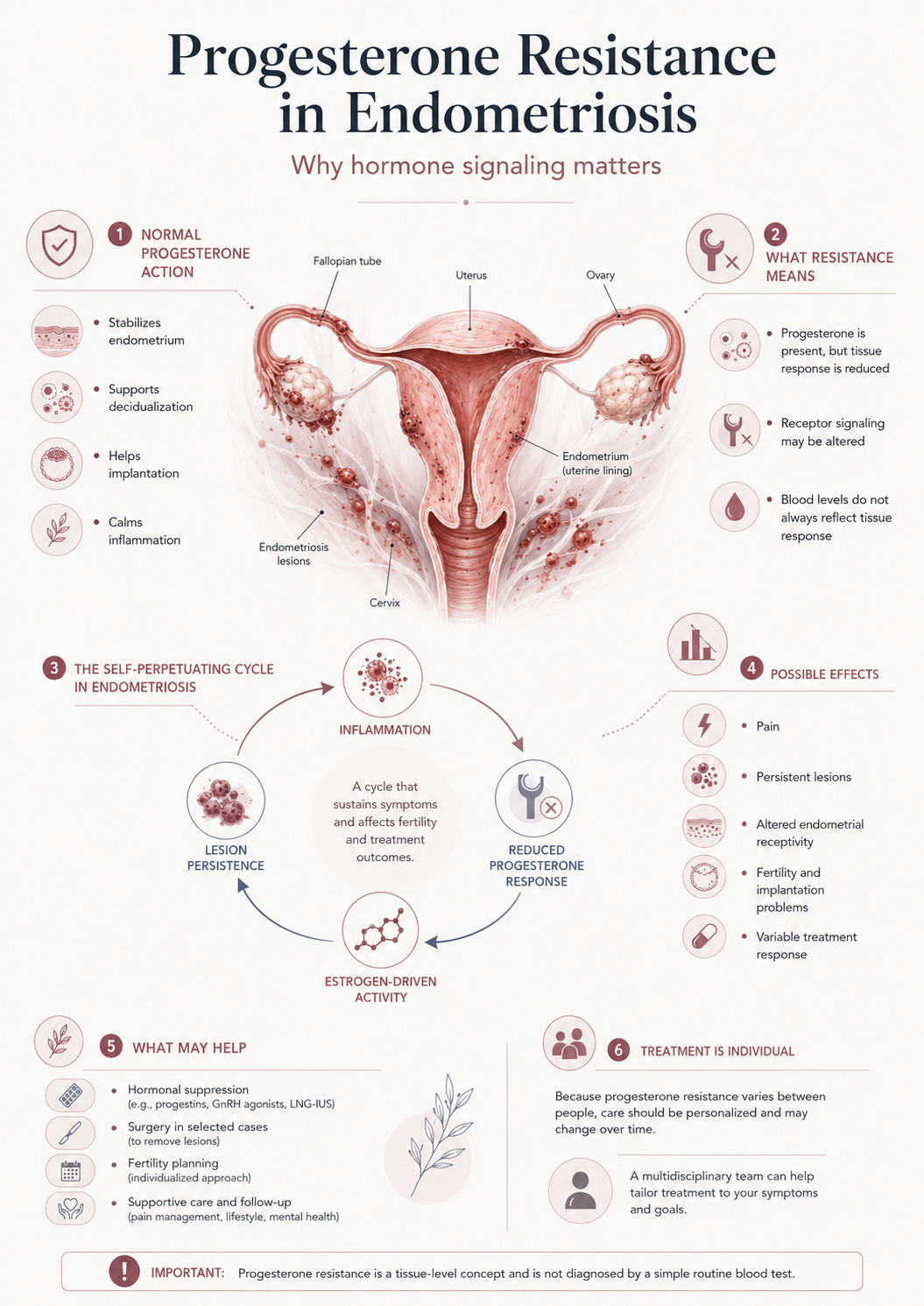
Progesterone resistance means that cells or tissues respond less effectively to progesterone signaling than expected. In endometriosis, this may help explain persistent inflammation, altered endometrial receptivity, pain, lesion survival, fertility problems and variable response to hormonal treatment.
This does not mean progesterone is useless.
It means the hormone signal may not be translated normally in some tissues.
That distinction matters.
What progesterone normally does
Progesterone rises after ovulation.
In a normal menstrual cycle, it helps transform the endometrium from a proliferative, estrogen-driven state into a secretory and pregnancy-ready state.
Progesterone helps regulate:
- endometrial maturation
- decidualization
- implantation readiness
- immune tolerance
- inflammatory balance
- uterine calmness
- menstrual control
- early pregnancy support
In simple terms:
Estrogen builds and stimulates.
Progesterone organizes, stabilizes and prepares.
This is simplified, but useful.
In a healthy cycle, estrogen and progesterone should not be seen as enemies. They are part of a coordinated system.
In endometriosis, this coordination may be disturbed.
What is progesterone resistance?
Progesterone resistance means that the biological response to progesterone is reduced, altered or incomplete.
The body may produce progesterone. Progesterone may be present in the blood. But the target tissue may not respond normally.
This can happen through several mechanisms, including:
- altered progesterone receptor expression
- abnormal progesterone receptor signaling
- chronic inflammation
- epigenetic changes
- altered gene expression
- oxidative stress
- estrogen dominance at the tissue level
- changes in immune cell behavior
- environmental or metabolic influences under investigation
In endometriosis, research describes increasing evidence for impaired progesterone signaling and possible progesterone resistance, although the mechanisms are complex and still being studied.
The important point is this:
A normal progesterone level does not always guarantee normal progesterone action at the tissue level.
Why progesterone resistance matters in endometriosis
Endometriosis is an estrogen-responsive inflammatory disease.
Progesterone would normally help limit some estrogen-driven growth and inflammatory activity. If progesterone signaling is weaker, estrogen-driven and inflammatory processes may become harder to control.
Progesterone resistance may contribute to:
- persistence of endometriosis lesions
- continued inflammatory signaling
- impaired decidualization
- altered uterine receptivity
- heavier or painful cycles
- reduced response to progestin treatment in some patients
- fertility and implantation problems
- recurrence tendency after treatment
- difficulty achieving long-term symptom control
This does not mean every patient with endometriosis has the same level of progesterone resistance.
It means progesterone resistance may be one important mechanism within the broader disease system.
The receptor problem: hearing the hormone signal
Hormones work by binding to receptors.
If progesterone is the message, the progesterone receptor is the receiving system.
Endometriosis research has focused on altered expression and function of progesterone receptors, especially changes in receptor isoforms and downstream signaling.
If the receptor system is abnormal, the tissue may not “hear” the progesterone message clearly.
This may result in a state where progesterone is present, but the expected anti-inflammatory, stabilizing or differentiation effects are reduced.
This is one reason why endometriosis cannot be understood only through blood hormone levels.
The tissue response matters.
Inflammation and progesterone resistance reinforce each other
Inflammation and progesterone resistance may form a loop.
Chronic inflammation may interfere with progesterone signaling. Reduced progesterone response may then allow more inflammation to persist.
This creates a possible self-reinforcing pattern:
Inflammation
↓
Reduced progesterone response
↓
Less control of estrogen-driven activity
↓
More lesion survival and inflammatory signaling
↓
More inflammation
This loop is one reason endometriosis can be persistent.
It is also why treatment may require more than simply adding or suppressing hormones. The inflammatory tissue environment may matter.
Estrogen, aromatase and local hormone production
Endometriosis lesions may create a local hormonal environment that supports their own survival.
Some lesions have been associated with increased local estrogen production through aromatase activity. Estrogen can promote inflammation, lesion growth and pain signaling.
If progesterone signaling is impaired at the same time, the balance shifts further toward estrogen-driven activity.
This is sometimes described as local estrogen dominance, but the phrase should be used carefully.
It does not always mean high estrogen in the blood.
It may mean that the local tissue environment behaves as if estrogen stimulation is strong and progesterone counter-regulation is weak.
This is why systemic blood tests may not fully explain endometriosis behavior.
Progesterone resistance and fertility
Progesterone is essential for implantation.
After ovulation, the endometrium must become receptive. If pregnancy begins, it must transform into decidua, the specialized pregnancy-supporting tissue.
If progesterone response is impaired, this may affect:
- endometrial receptivity
- implantation timing
- decidualization
- immune tolerance
- early placental communication
- inflammatory balance
- early pregnancy stability
This does not mean progesterone resistance explains all infertility in endometriosis.
Endometriosis-related infertility may also involve pelvic anatomy, adhesions, ovarian endometriomas, ovarian reserve, inflammation, egg quality, sperm-egg interaction, adenomyosis and embryo factors.
But progesterone resistance gives a coherent link between endometriosis, inflammation and implantation biology.
Why progesterone treatment may help some women but not all
Many endometriosis treatments use progesterone-like effects.
These may include:
- progestin tablets
- hormonal intrauterine systems
- combined hormonal contraceptives
- continuous hormonal suppression
- IVF luteal support in fertility treatment
These approaches can reduce bleeding, suppress cycling, lower estrogen-driven stimulation and reduce symptoms in many patients.
But response varies.
Some women improve dramatically. Others have partial benefit. Some cannot tolerate side effects. Some continue to have pain despite suppression.
Progesterone resistance may be one possible reason for variable response, but it is not the only reason.
Other reasons include:
- deep infiltrating disease
- adhesions and fibrosis
- nerve sensitization
- pelvic floor dysfunction
- bowel or bladder involvement
- adenomyosis
- central pain amplification
- incomplete suppression
- individual pharmacological differences
This is why treatment response should be monitored rather than assumed.
Does progesterone resistance mean progesterone treatment will not work?
No.
This is a common misunderstanding.
Progesterone resistance does not mean progesterone treatment is always useless.
It means that the response may be altered, incomplete or different between tissues and patients.
Some women with endometriosis respond well to progestin-based therapy. Others need different strategies. Some need surgery. Some need multidisciplinary pain care. Some need fertility-focused planning.
The presence of progesterone resistance as a concept should not lead to fatalism.
It should lead to better interpretation.
Can progesterone resistance be tested?
In routine clinical care, there is usually no simple blood test that tells a patient whether she has progesterone resistance in her endometriosis tissue.
This is important.
Blood progesterone can be measured, especially in fertility contexts, but blood levels do not directly prove how endometriosis lesions or the endometrium respond at the cellular level.
Progesterone resistance is mainly a tissue-level and molecular concept.
Research may study:
- progesterone receptor expression
- gene expression patterns
- inflammatory markers
- epigenetic changes
- endometrial response
- lesion biology
- decidualization markers
But these are not yet standard everyday tools for most patients.
So clinically, progesterone resistance is usually inferred from the disease biology and treatment patterns, not directly measured.
What can be done if progesterone signaling is impaired?
There is no single “progesterone resistance reversal” treatment used routinely in endometriosis care.
But several strategies may help reduce the impact of the disease.
Hormonal suppression
Progestins, combined hormonal contraceptives, GnRH agonists or antagonists and other hormonal strategies may reduce cycling, estrogen stimulation and symptoms.
The goal is often not to “fix” progesterone resistance directly, but to suppress the disease environment.
Surgery in selected cases
When deep disease, endometriomas, organ involvement or severe symptoms are present, specialist surgery may be considered. Surgery may reduce lesion burden, but it does not automatically correct the underlying inflammatory tendency.
Fertility strategy
In fertility care, progesterone support may be used according to IVF protocols or luteal phase needs. But implantation outcomes depend on more than progesterone alone.
Inflammation-aware supportive care
Sleep, metabolic health, gut symptoms, stress physiology, physical activity, nutrient status and inflammatory load may all influence overall resilience. These strategies should not be presented as cures, but they may reduce symptom burden or improve general health context.
Individualized treatment monitoring
Because response varies, treatment should be evaluated over time:
Are symptoms improving?
Is bleeding controlled?
Is pain reduced?
Are side effects acceptable?
Are fertility goals changing?
Is surgery needed?
Is another diagnosis also present?
The key is not one intervention.
The key is structured follow-up.
What not to overclaim
Progesterone resistance is an important concept, but it can easily be misused.
It should not be used to claim:
- all endometriosis is caused by low progesterone
- progesterone supplements cure endometriosis
- blood progesterone level explains the whole disease
- every woman with endometriosis needs progesterone
- progesterone resistance can be diagnosed from symptoms alone
- diet or supplements can reliably reverse progesterone resistance
- failed implantation is always caused by progesterone resistance
These claims are too strong.
A more accurate statement is:
Progesterone resistance is one important mechanism that may help explain inflammation, lesion persistence, altered receptivity and treatment variability in endometriosis. But it is part of a larger disease system.
Why this matters for High Coast Women’s Health Intelligence
Progesterone resistance is exactly the type of concept that needs better patient education.
It sits between:
- hormone health
- inflammation
- fertility
- implantation
- pregnancy support
- treatment response
- biomarker limitations
- research and clinical uncertainty
It helps explain why “normal labs” may not mean normal tissue response.
It also helps explain why endometriosis needs a systems model, not a one-hormone explanation.
Key message
Progesterone resistance means that tissue may respond less effectively to progesterone signaling.
In endometriosis, this may contribute to inflammation, lesion persistence, altered endometrial receptivity, fertility problems and variable treatment response.
But progesterone resistance does not mean progesterone is irrelevant, and it does not mean treatment cannot work.
The more useful view is this:
Endometriosis is not only about hormone levels.
It is about how tissues respond to hormone signals in an inflammatory environment.
That is why hormone health, immune signaling and tissue biology must be interpreted together.
- Progesterone Resistance in Endometriosis: Current Evidence and Putative Mechanisms International Journal of Molecular Sciences / MDPI
Review focused on the evidence and proposed mechanisms of progesterone resistance in endometriosis, including receptor signaling, inflammation, gene expression and epigenetic changes - Endometriosis guideline ESHRE — European Society of Human Reproduction and Embryology
Best-practice guideline for diagnosis and management of endometriosis, including pain treatment, infertility and medically assisted reproduction - ESHRE guideline: endometriosis Human Reproduction Open / Oxford Academic
Published summary of the ESHRE guideline with evidence-based recommendations for medical treatment, surgery and assisted reproduction - Endometriosis: diagnosis and management NICE — National Institute for Health and Care Excellence
Guideline covering diagnosis and management of endometriosis, including symptoms, referral, treatment options and fertility-priority care - Endometriosis and the Role of Pro-Inflammatory and Anti-Inflammatory Cytokines in Pathophysiology NIH PMC / Diagnostics
Review of inflammatory mechanisms in endometriosis, including cytokines, immune signaling, oxidative stress and possible biomarker relevance
