A structured overview of progesterone as a tissue-signal hormone
Progesterone is often described as a female sex hormone or a pregnancy hormone.
That is true, but incomplete.
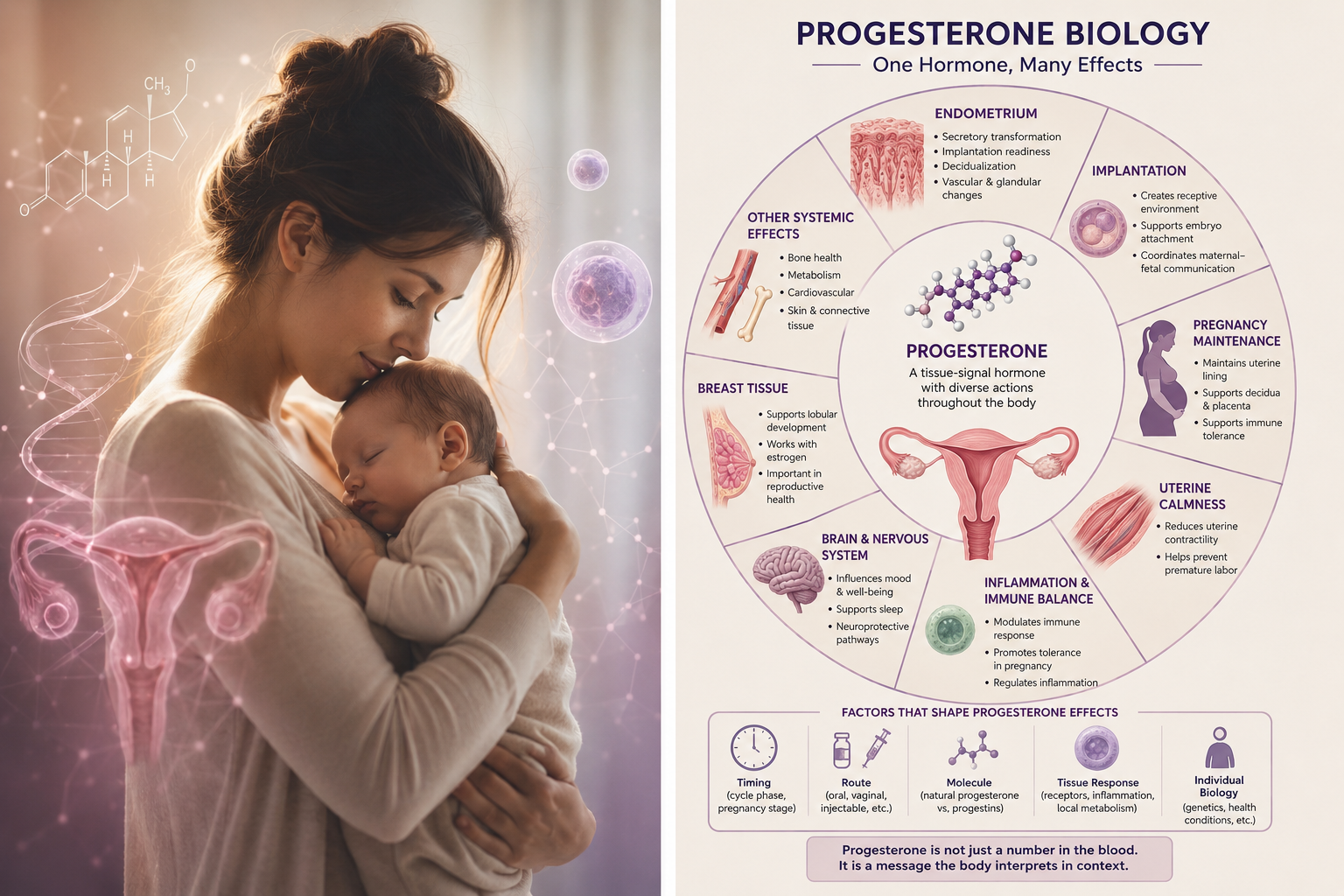
Progesterone is better understood as a tissue-signal hormone. Its effects depend on timing, dose, route, receptor expression, tissue state, inflammation, local metabolism and whether the target tissue can respond appropriately.
This is why progesterone can appear simple in theory but complicated in practice.
In one context, progesterone supports implantation.
In another, it helps maintain pregnancy.
In another, it reduces uterine contractility.
In another, it influences immune tolerance.
In another, it may affect sleep, mood or nervous system function.
In another, progesterone-like molecules may behave differently from natural progesterone.
So the important question is not only:
Is progesterone present?
The deeper question is:
Where is progesterone acting, when is it acting, and how is the tissue responding?
This article gives a structured overview of progesterone biology without assuming that progesterone is a universal solution. The evidence should lead the conclusion, not the other way around.
What is progesterone?
Progesterone is a steroid hormone produced mainly by the corpus luteum after ovulation and later by the placenta during pregnancy.
It is also produced in smaller amounts by the adrenal glands and can act in several tissues beyond the reproductive organs.
In reproductive biology, progesterone is central because it helps shift the body from an estrogen-driven growth phase into a more organized, secretory, stabilizing and pregnancy-supportive phase.
In a simplified model:
Estrogen builds and stimulates.
Progesterone organizes, differentiates and stabilizes.
That simplification is useful, but progesterone biology is more complex than a simple “estrogen versus progesterone” story.
Progesterone does not work alone. It interacts with estrogen, cortisol, immune signaling, thyroid function, metabolic state, tissue receptors and local inflammatory conditions.
Progesterone in the menstrual cycle
After ovulation, the empty follicle becomes the corpus luteum. The corpus luteum produces progesterone.
This rise in progesterone changes the endometrium, the lining inside the uterus.
The endometrium moves from a proliferative phase into a secretory phase. It becomes more prepared for possible implantation.
If pregnancy does not occur, progesterone falls. This fall helps trigger menstruation.
If pregnancy occurs, progesterone remains important. It supports the endometrium, helps maintain early pregnancy and contributes to the transformation of the uterine lining into decidua.
This is why the timing of progesterone matters.
A progesterone value means different things depending on cycle day, ovulation timing, pregnancy status and tissue context.
Progesterone and the endometrium
The endometrium is one of progesterone’s most important target tissues.
Progesterone helps regulate:
- secretory transformation
- implantation readiness
- decidualization
- local immune balance
- endometrial gland function
- stromal cell differentiation
- vascular changes
- menstrual stability
Decidualization is especially important. It is the process where endometrial stromal cells transform into specialized pregnancy-supporting decidual cells.
This process is essential for implantation and early placental development.
In other words, progesterone does not simply “thicken” the lining. It changes what the lining becomes.
That difference matters.
A thick endometrium is not automatically a receptive endometrium.
A normal blood progesterone value is not automatically proof of perfect tissue response.
The biological response inside the tissue is what ultimately matters.
Progesterone and implantation
Implantation requires coordination between the embryo and the uterine lining.
The endometrium must be receptive at the right time. Immune cells must be regulated. Blood vessels must remodel. Inflammatory signals must be balanced. The embryo must communicate with the maternal tissue.
Progesterone helps prepare this environment.
It supports:
- receptivity
- decidualization
- immune tolerance
- vascular adaptation
- early maternal-fetal communication
- reduction of excessive inflammatory activity
But implantation is not controlled by progesterone alone.
Embryo quality, timing, uterine anatomy, adenomyosis, endometriosis, inflammation, thyroid status, metabolic health and other factors can all matter.
Progesterone is central, but not omnipotent.
That is a useful starting point for serious discussion.
Progesterone and pregnancy maintenance
During early pregnancy, progesterone helps maintain the uterine environment.
It supports the decidua, contributes to immune tolerance and helps keep the uterus in a less contractile state.
Later in pregnancy, the placenta becomes the major source of progesterone.
Progesterone is involved in several pregnancy-related processes:
- maintaining the uterine lining
- supporting decidual tissue
- reducing uterine contractility
- modulating maternal immune activity
- supporting placental function
- helping maintain pregnancy continuity
This is why progesterone has been studied in contexts such as threatened miscarriage, recurrent miscarriage, IVF luteal support and preterm birth prevention.
But clinical use is not the same as biological importance.
A hormone can be biologically essential without every supplementation strategy producing strong clinical benefit in every patient group.
That is one of the central lessons of progesterone research.
Progesterone and immune tolerance
Pregnancy requires a special immune balance.
The maternal immune system must tolerate the embryo and placenta, which contain genetic material from the father, while still protecting against infection.
Progesterone is one of the hormones involved in this balance.
It can influence immune cells, cytokine production, inflammatory signaling and maternal-fetal tolerance. It is active not only in the endometrium, but also in the decidua, placenta, myometrium and maternal circulation.
This immunological role is one reason progesterone is so interesting.
It may help explain why progesterone is relevant to implantation, early pregnancy, inflammation, endometriosis, miscarriage research and pregnancy complications.
But immune modulation is complex. More progesterone is not automatically better.
The right biological effect depends on context.
Progesterone and uterine calmness
Progesterone helps maintain uterine quiescence, meaning a state where the uterus remains relatively calm and less contractile during pregnancy.
This matters because pregnancy requires the uterus to expand without contracting too early.
Progesterone influences the myometrium, the muscular wall of the uterus, and interacts with pathways involved in contractility and labor timing.
This is one reason progesterone has been studied in preterm birth prevention.
However, preterm birth is not one single condition. It can involve cervical factors, infection, inflammation, uterine overdistension, placental problems, previous preterm birth, bleeding, multiple pregnancy and other mechanisms.
So progesterone may help in some contexts and not others.
Again, the biology is important, but patient selection matters.
Progesterone and inflammation
Progesterone is often described as anti-inflammatory, but that phrase needs care.
Inflammation is not always harmful. Controlled inflammatory signaling is necessary for ovulation, implantation, placental development and tissue remodeling.
The problem is not inflammation itself. The problem is excessive, mistimed or poorly regulated inflammation.
Progesterone can help shift immune and inflammatory responses toward a pregnancy-supportive environment.
But it does not simply “turn off inflammation.”
A more accurate statement is:
Progesterone helps regulate inflammatory and immune signaling in reproductive tissues, especially in contexts where tissue tolerance, implantation and pregnancy maintenance are required.
This is why progesterone is relevant to endometriosis, miscarriage research and pregnancy support — but not a universal anti-inflammatory treatment.
Progesterone beyond reproduction
Progesterone also acts outside the uterus.
It may influence:
- brain and nervous system function
- sleep physiology
- mood regulation
- breast tissue
- bone and vascular biology
- metabolism
- skin and connective tissue
- immune responses
Some progesterone metabolites interact with GABA-related pathways in the nervous system, which may help explain why progesterone can affect sleepiness or calmness in some contexts.
However, systemic effects vary depending on route, formulation, dose, individual metabolism and whether natural progesterone or a synthetic progestin is used.
This is why it is risky to speak about “progesterone” as if every molecule with progestogenic activity behaves identically.
Natural progesterone and synthetic progestins are not the same thing
This is a critical point.
Natural progesterone is structurally identical to the progesterone produced by the body.
Synthetic progestins are molecules designed to activate progesterone-related pathways, but they are not identical to natural progesterone. Different progestins can have different activity at progesterone receptors and may also interact with androgen, glucocorticoid or mineralocorticoid pathways depending on their structure.
This means “progesterone-like” does not always mean “same biological effect.”
For clinical discussion, the umbrella term is often progestogens.
Progestogens include:
- natural progesterone
- synthetic progestins
This distinction matters in contraception, menopausal hormone therapy, fertility treatment, pregnancy support and endometriosis treatment.
A treatment study using one progestin should not automatically be interpreted as evidence for natural progesterone, and vice versa.
The molecule matters.
Route matters: oral, vaginal, injectable and local exposure
Progesterone effects depend not only on the molecule, but also on how it is delivered.
Different routes can produce different exposure patterns:
- oral progesterone
- vaginal progesterone
- intramuscular progesterone
- subcutaneous progesterone
- intrauterine progestin delivery
- transdermal or topical routes in some contexts
Oral progesterone undergoes first-pass metabolism in the liver, which can increase certain metabolites and influence sedation or systemic effects.
Vaginal progesterone may produce different uterine exposure than serum levels alone suggest.
Injectable progesterone may create different systemic levels and duration.
Intrauterine delivery of a progestin may create strong local endometrial effects with lower systemic exposure.
This is where progesterone becomes a pharmacokinetic and tissue-distribution problem, not only a hormone-level problem.
The same nominal hormone can behave differently depending on route.
Timing matters
Progesterone is highly timing-dependent.
It matters whether progesterone rises:
- before ovulation
- after ovulation
- during the implantation window
- after embryo transfer
- in early pregnancy
- in mid-pregnancy
- near labor
- during perimenopause
- after menopause
In fertility and pregnancy support, timing can be especially important.
Too little progesterone at the wrong time may be a problem. But progesterone exposure that is mistimed may also affect endometrial synchrony.
The endometrium is not only asking “how much hormone?”
It is asking:
Is the signal arriving at the right time?
This is one reason dynamic progesterone biology is more meaningful than a single static measurement.
Tissue response matters
Progesterone works through receptors and downstream signaling.
If a tissue does not express the right receptors, or if receptor signaling is altered, progesterone may not produce the expected effect.
This is important in endometriosis, where progesterone resistance has been proposed as a key mechanism.
It is also important in broader reproductive medicine because tissue-level response may not be fully captured by serum hormone levels.
A blood test can tell us what is circulating. It does not automatically tell us what is happening inside a specific region of the endometrium, decidua, cervix, myometrium or lesion.
This is a major limitation of oversimplified progesterone thinking.
The real biology is:
Hormone level
↓
Tissue delivery
↓
Receptor expression
↓
Cellular response
↓
Functional effect
Every step can vary.
Why progesterone studies can be difficult to interpret
Progesterone research often produces mixed results.
This does not necessarily mean progesterone is unimportant. It may mean that studies group together patients whose biology is not the same.
Clinical outcomes may depend on:
- indication
- gestational age
- route
- dose
- timing
- baseline progesterone level
- tissue response
- previous miscarriage history
- IVF protocol
- cervical length
- inflammation
- endometriosis or adenomyosis
- embryo quality
- multiple pregnancy
- molecular differences between progesterone and progestins
If a trial includes many different mechanisms under one label, the result may look weak even if a subgroup benefits.
This is why the future of progesterone research should probably move toward more individualized and mechanism-based models.
The question is not simply:
Does progesterone work?
The better question is:
For which tissue state, which patient group, which route, which timing and which outcome?
Why progesterone is not a miracle medicine
Progesterone is biologically powerful.
But powerful does not mean universal.
It is not scientifically responsible to say that progesterone can solve every case of miscarriage risk, implantation failure, endometriosis, inflammation, pregnancy bleeding or preterm birth risk.
Those conditions have many different causes.
Progesterone may be highly relevant in some contexts and less relevant in others.
The strongest position is not advocacy.
The strongest position is precision:
Understand the biology.
Respect the evidence.
Separate natural progesterone from progestins.
Separate serum levels from tissue effects.
Separate established clinical use from hypothesis.
Study timing, route, dose and tissue response more carefully.
That is where progesterone biology becomes intellectually serious.
What better progesterone research may need
Future progesterone research may need to move beyond simple treatment-versus-placebo thinking.
More advanced research could include:
- dynamic serum progesterone measurements
- route-specific pharmacokinetics
- local uterine exposure models
- tissue receptor mapping
- endometrial and decidual biomarkers
- spatial transcriptomics
- inflammation markers
- progesterone response markers
- better subgroup classification
- fertility and pregnancy outcome linkage
- AI-supported pattern analysis
The goal should not be to prove that progesterone is always good or always ineffective.
The goal should be to understand when progesterone biology matters, when treatment helps, when it fails, and why.
Key message
Progesterone is not just a pregnancy hormone.
It is a tissue-signal hormone that affects the endometrium, decidua, immune system, uterus, placenta, nervous system and other tissues.
Its effects depend on timing, route, molecule, receptor expression, local tissue state and biological context.
This is why progesterone can be both essential and difficult to study.
The serious question is not whether progesterone is a miracle medicine.
The serious question is how progesterone signaling works in specific tissues, at specific times, in specific patients — and how evidence can guide better use.
- Progesterone-Regulated Endometrial Factors Controlling Implantation American Journal of Reproductive Immunology / NIH PMC
Review of progesterone receptor action in uterine function, implantation and early gestation.
- Progesterone: A Unique Hormone with Immunomodulatory Roles in Pregnancy International Journal of Molecular Sciences / NIH PMC
Review of progesterone’s endocrine and immunomodulatory roles in pregnancy, including immune tolerance and inflammatory regulation.
- The Effects of Progesterone on Immune Cellular Function at the Maternal-Fetal Interface and Maternal Circulation Journal of Steroid Biochemistry and Molecular Biology / NIH PMC
Review of progesterone’s effects on immune cells in the decidua, placenta, myometrium and maternal circulation.
- Progesterone-Related Immune Modulation of Pregnancy and Labor Frontiers in Endocrinology
Review of progesterone pathways in maternal reproductive and immune systems, including inflammation and labor.
- Progesterone Resistance in Endometriosis: Current Evidence and Putative Mechanisms International Journal of Molecular Sciences / MDPI
Review of progesterone resistance in endometriosis, relevant to receptor signaling, inflammation, fertility and treatment response.
