
Why midlife hormone change is also a shift in cardiovascular, inflammatory and metabolic risk
Menopause is often described as a hormonal milestone. In everyday language, it is associated with hot flashes, night sweats, sleep disruption, cycle irregularity, mood changes, vaginal dryness and the final menstrual period.
But biologically, menopause is much more than the end of reproductive cycling.
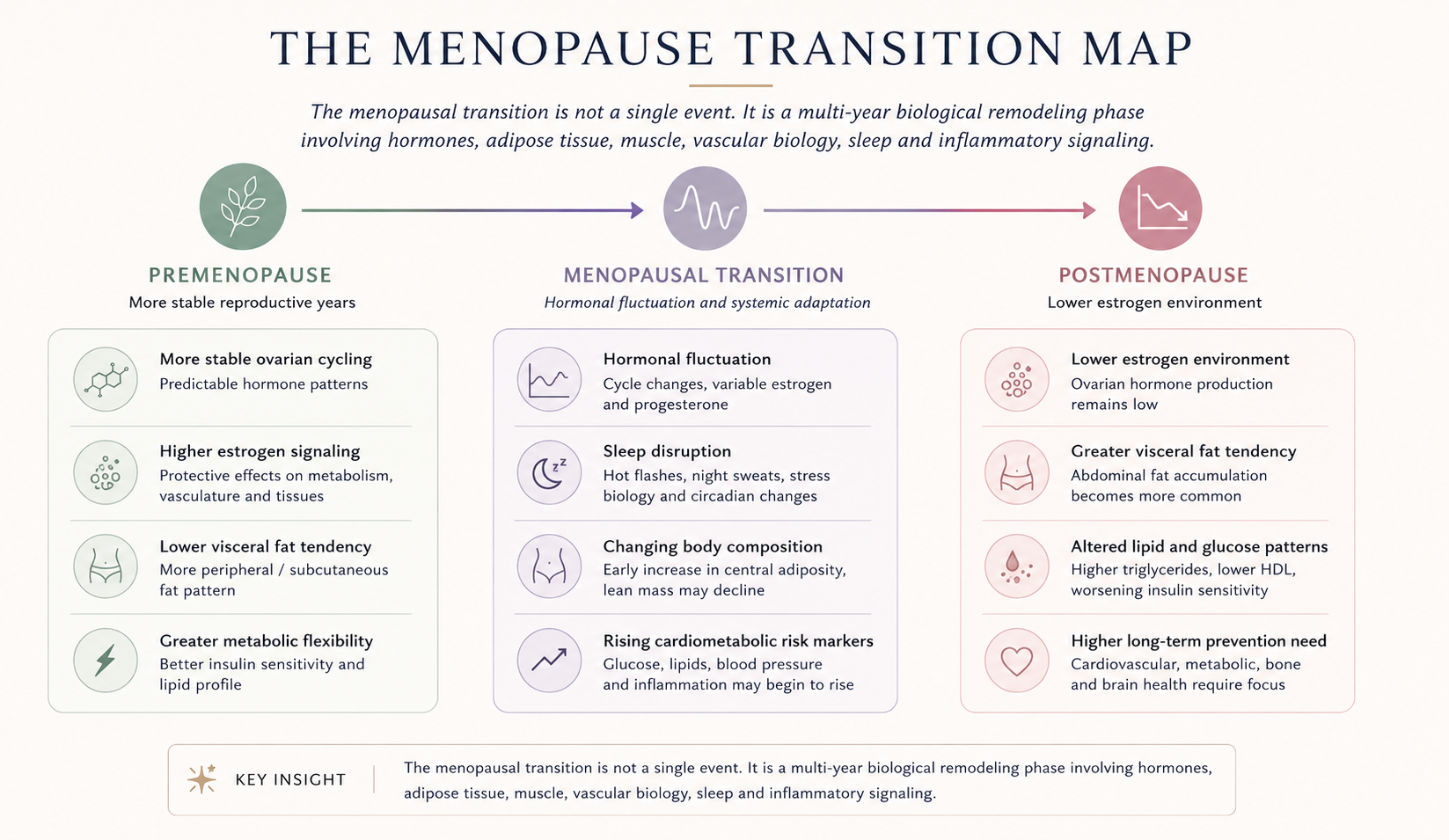
The menopausal transition is a multi-year remodeling phase in women’s health. During this period, ovarian hormone patterns become more variable, estrogen levels eventually decline, body composition begins to shift, visceral fat may increase, insulin sensitivity can worsen, lipid profiles often become less favorable, vascular risk begins to rise, and inflammatory signaling may become more prominent.
This does not mean that menopause is a disease. It means that menopause is a biological transition point where reproductive aging, metabolic regulation and long-term health risk begin to interact more strongly.
The central insight is this:
Menopause should not only be understood as a hormonal transition. It should also be understood as a metabolic transition.
That shift in perspective matters. It changes the question from:
How do we treat menopause symptoms?
to:
How do we protect metabolic resilience during and after the menopausal transition?
1. Menopause is not a single moment
Menopause is technically defined after twelve consecutive months without a menstrual period, but the biological transition begins earlier. The years leading up to the final menstrual period are often called the menopausal transition or perimenopause.
During this phase, hormone patterns may fluctuate substantially. Estrogen does not simply decline in a smooth straight line. Instead, levels can vary, cycles become less predictable, and the body gradually adapts to a new endocrine environment.
This matters because the metabolic effects of menopause are not limited to the moment menstruation stops. Changes in sleep, body composition, vascular function, lipids, glucose regulation and inflammation may begin during the transition itself.
A useful way to think about menopause is therefore not as an on/off switch, but as a biological slope.
The final menstrual period is one visible marker. The deeper process is systemic remodeling.
2. The deeper issue is metabolic resilience
Metabolic resilience is the body’s ability to maintain healthy regulation of energy, glucose, fat storage, vascular function and inflammatory balance under changing biological conditions.
Before menopause, estrogen signaling contributes to several protective patterns in the body. It influences fat distribution, vascular tone, lipid metabolism, glucose handling, bone biology, thermoregulation and possibly mitochondrial function.
After menopause, the body must regulate these systems in a lower-estrogen environment.
For some women, this transition is relatively smooth. For others, it is associated with weight gain, increasing waist circumference, rising blood pressure, worsening cholesterol patterns, insulin resistance, fatigue, sleep disturbance and inflammatory symptoms.
The important point is that menopause does not act alone. It interacts with:
- chronological aging
- genetics
- baseline body composition
- physical activity
- muscle mass
- diet
- sleep quality
- stress biology
- smoking history
- medication use
- social conditions
- previous pregnancy and reproductive history
This is why menopause should not be reduced to one hormone or one symptom. It is better understood as a systems-level transition.
3. Body fat distribution often changes
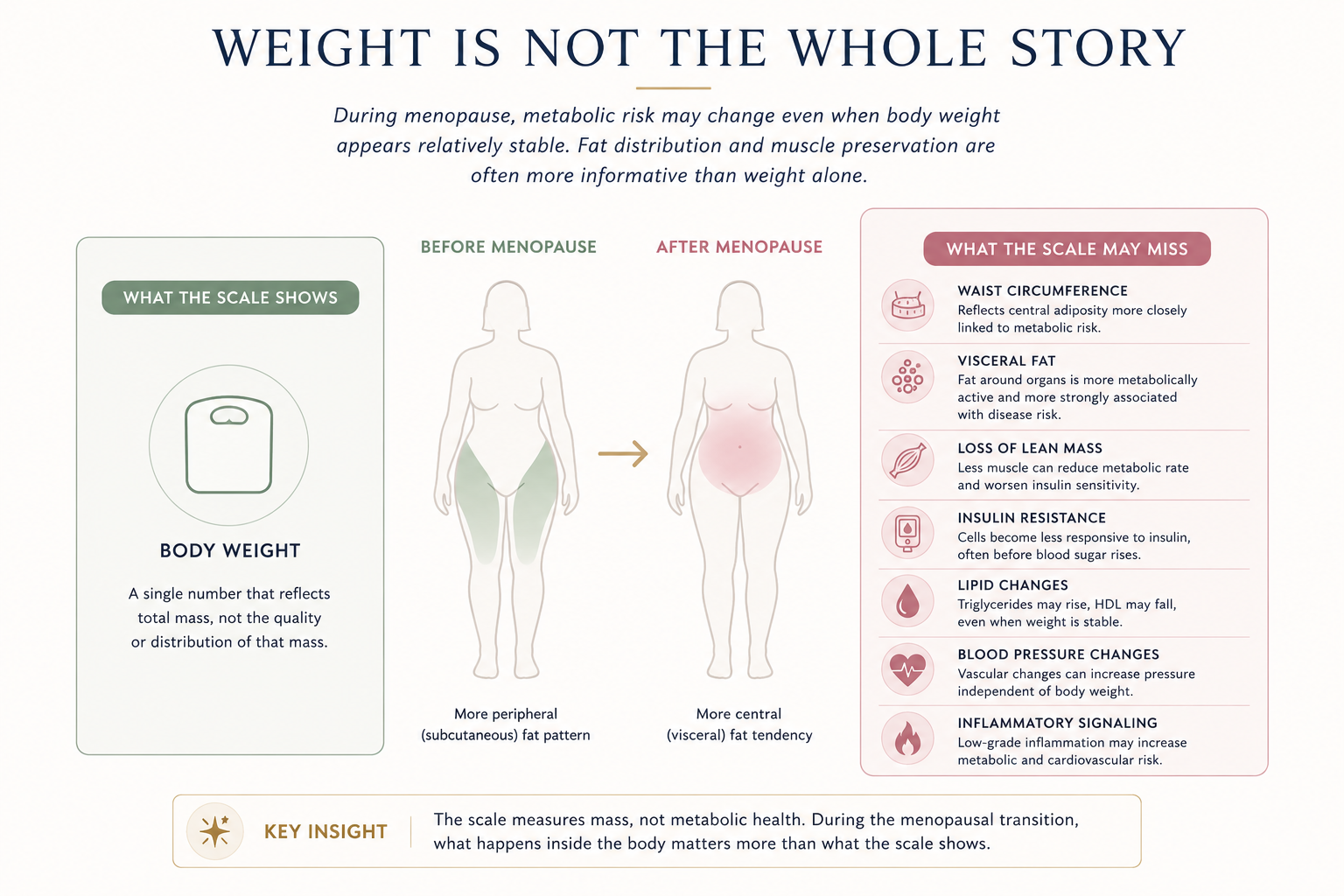
One of the most important metabolic changes around menopause is not simply weight gain. It is fat redistribution.
Many women notice that fat becomes easier to accumulate around the abdomen. Even when body weight changes only modestly, waist circumference may increase. This reflects a shift toward more central and visceral fat accumulation.
Visceral fat is the fat stored deeper in the abdomen around internal organs. It is more metabolically active than subcutaneous fat and is more strongly associated with insulin resistance, inflammation, dyslipidemia and cardiovascular risk.
This means that the scale can be misleading.
A woman may not gain a dramatic amount of weight, but her metabolic risk may still change if lean mass decreases and abdominal fat increases.
For this reason, menopause-related health assessment should not rely on BMI alone. Waist circumference, blood pressure, glucose markers, lipid markers and body composition trends often tell a more useful story.
4. Insulin sensitivity may decline
Insulin is the hormone that helps move glucose from the bloodstream into cells. When the body becomes less responsive to insulin, the pancreas must produce more insulin to maintain normal blood sugar. Over time, this can contribute to prediabetes, type 2 diabetes, fatty liver disease, metabolic syndrome and cardiovascular risk.
The menopausal transition can be associated with worsening insulin sensitivity, especially when it is combined with increased visceral fat, reduced muscle mass, poor sleep and reduced physical activity.
This is one reason why blood markers can begin to drift in midlife.
Fasting glucose may rise. HbA1c may slowly increase. Triglycerides may become less favorable. Waist circumference may increase. Blood pressure may move upward. These changes may occur gradually, long before a formal diagnosis is made.
This makes menopause an important prevention window.
The goal is not to wait until metabolic disease is established. The goal is to recognize the transition early enough to protect long-term resilience.
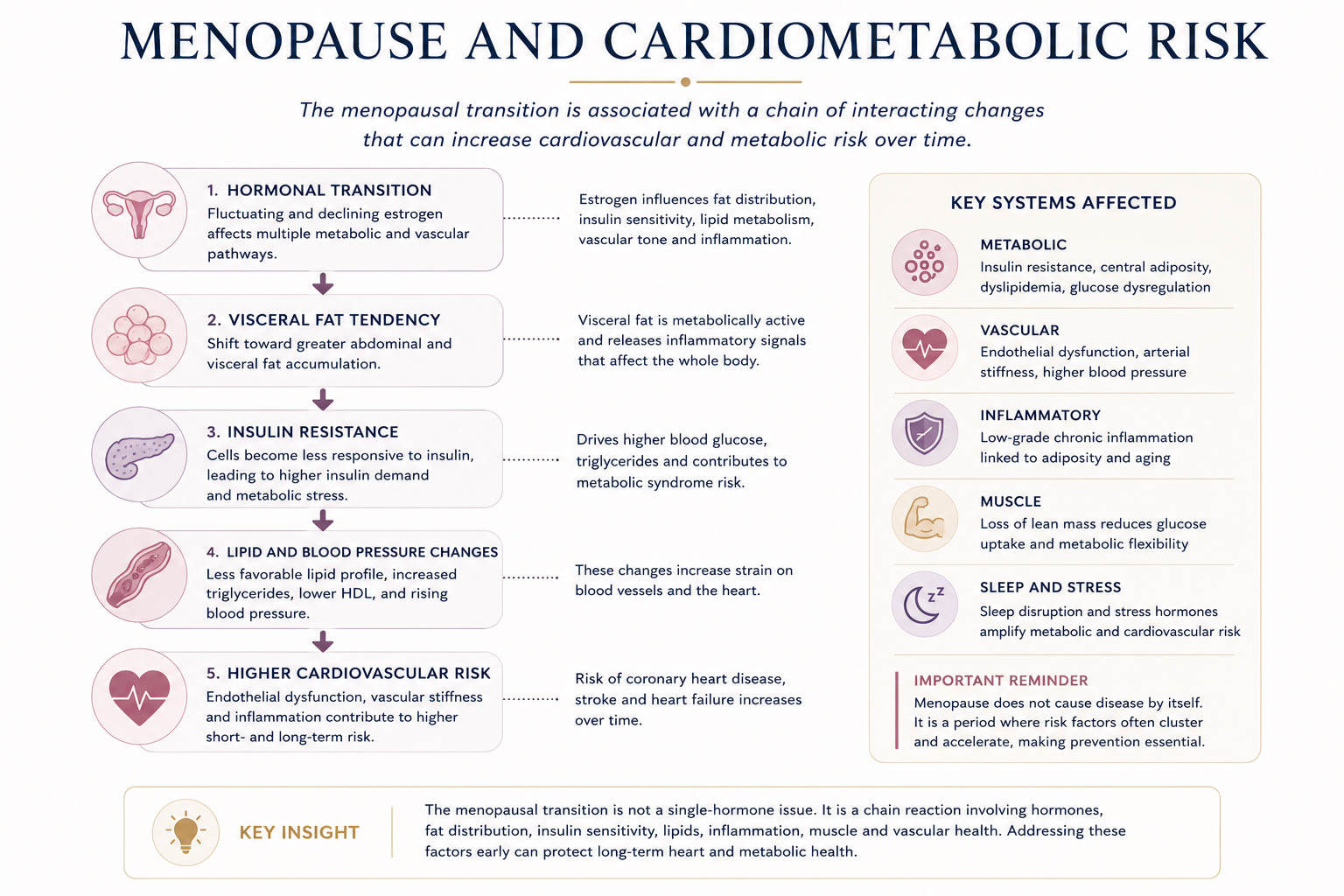
5. Cardiovascular risk becomes more visible
Cardiovascular disease is often thought of as a male health problem, but it is a major cause of illness and death in women. One reason it may be under-recognized is that women’s cardiovascular risk often accelerates later than men’s and may become more visible after midlife.
The menopausal transition is associated with several changes relevant to cardiovascular health:
- increased abdominal adiposity
- less favorable lipid profiles
- rising blood pressure
- changes in vascular stiffness
- changes in endothelial function
- increased insulin resistance
- increased inflammatory burden
This does not mean that menopause alone causes cardiovascular disease. Chronological aging remains important. But the menopausal transition appears to be a period where ovarian aging and general aging overlap in ways that can increase risk.
This is why menopause care should include cardiovascular prevention.
A serious menopause assessment should ask not only about hot flashes and cycle changes, but also about blood pressure, lipids, glucose regulation, waist circumference, family history, smoking, physical activity, sleep and inflammatory risk.
6. Muscle becomes more important after menopause
Muscle is often discussed in relation to strength and appearance, but it is also a major metabolic organ.
Skeletal muscle helps regulate glucose disposal, insulin sensitivity, energy use, posture, mobility and long-term independence. It also communicates with the immune system and contributes to metabolic flexibility.
During midlife and after menopause, preserving muscle becomes especially important. If lean mass declines while visceral fat increases, the body may become more insulin resistant even without dramatic weight gain.
This is why resistance training, adequate protein intake, physical activity and recovery are not cosmetic recommendations. They are metabolic interventions.
A menopause-focused health model should therefore treat muscle as a core prevention target.
The goal is not simply weight control. The goal is to preserve metabolically active tissue.
7. Sleep can amplify metabolic change
Sleep disruption is one of the most common and underestimated problems during the menopausal transition.
Hot flashes, night sweats, anxiety, mood changes, stress and changing circadian patterns can all disturb sleep. Poor sleep can then worsen appetite regulation, glucose metabolism, blood pressure, inflammation and stress hormone patterns.
This creates a loop:
hormonal fluctuation → sleep disruption → metabolic stress → more fatigue and weight gain tendency → reduced resilience
Sleep is therefore not just a quality-of-life issue. It is part of metabolic regulation.
In a modern menopause model, sleep should be evaluated alongside hormones, glucose, lipids, blood pressure, body composition and mental health.
8. Inflammation connects many of the changes
Inflammation is one of the biological bridges between visceral fat, insulin resistance, vascular risk and aging.
Visceral adipose tissue is not just passive fat storage. It can release inflammatory signals that affect insulin sensitivity, endothelial function, liver metabolism and immune regulation.
At the same time, aging itself is associated with a gradual increase in low-grade inflammatory activity. When this age-related inflammatory tendency overlaps with menopause-related body composition change, cardiometabolic risk may increase.
This is why menopause is not only an endocrine topic. It is also an immune-metabolic topic.
A strong women’s health intelligence model should therefore include inflammatory markers and inflammatory pathways in the way menopause is understood.
9. Hormone therapy: important, but not the whole answer
Menopausal hormone therapy can be highly effective for vasomotor symptoms such as hot flashes and night sweats. It is also relevant for genitourinary syndrome of menopause and bone health. For many healthy symptomatic women under 60 years of age or within 10 years of menopause onset, major menopause societies describe the benefit-risk balance as favorable when treatment is individualized.
But hormone therapy should not be presented as a universal metabolic solution.
The risks and benefits depend on age, time since menopause, symptoms, personal risk factors, dose, formulation, route of administration, whether the uterus is present, and whether a progestogen is needed.
For metabolic health, the most responsible position is this:
Hormone therapy may be part of individualized menopause care, but metabolic prevention should never depend on hormones alone.
A prevention-centered menopause model should include body composition, muscle, sleep, blood pressure, lipids, glucose regulation, inflammation, nutrition, physical activity and cardiovascular risk assessment.
Hormones matter. But they are not the whole system.
10. Menopause as a prevention window
The most important clinical and public health message is that menopause is a window of opportunity.
It is a time when risk markers may begin to change, but before disease is necessarily established. That creates an opportunity for early intervention.
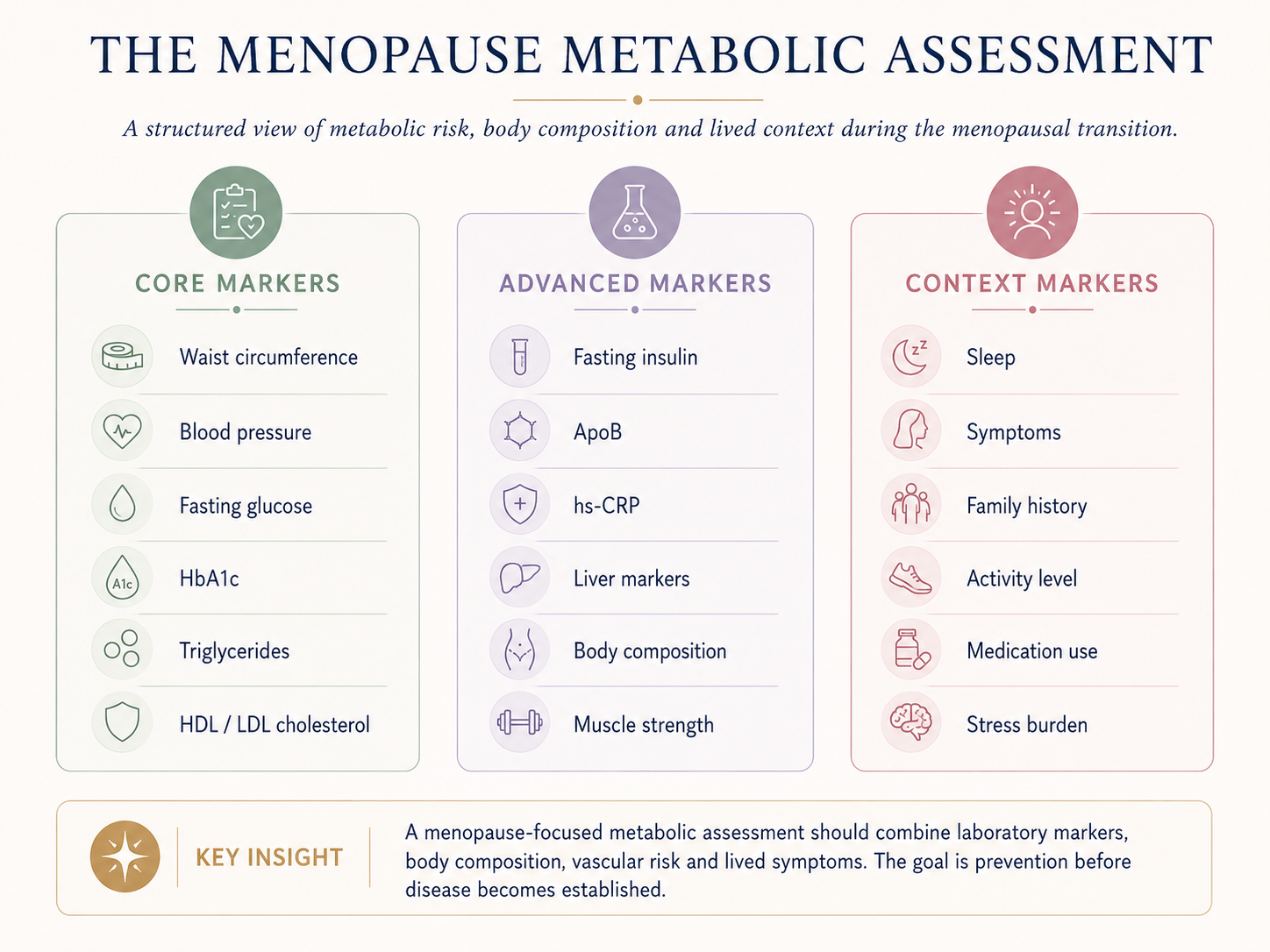
A menopause metabolic assessment should consider:
- waist circumference
- blood pressure
- fasting glucose
- HbA1c
- fasting insulin, when appropriate
- triglycerides
- HDL cholesterol
- LDL cholesterol
- ApoB, when available
- hs-CRP, when clinically relevant
- liver markers
- body composition
- muscle strength
- sleep quality
- vasomotor symptoms
- family history
- smoking status
- physical activity
- medication history
The most useful approach is longitudinal. A single blood test can be helpful, but trends over time are often more informative.
The key question is not only: “Are the values normal today?”
The better question is:
In which direction is this person’s metabolic risk moving?
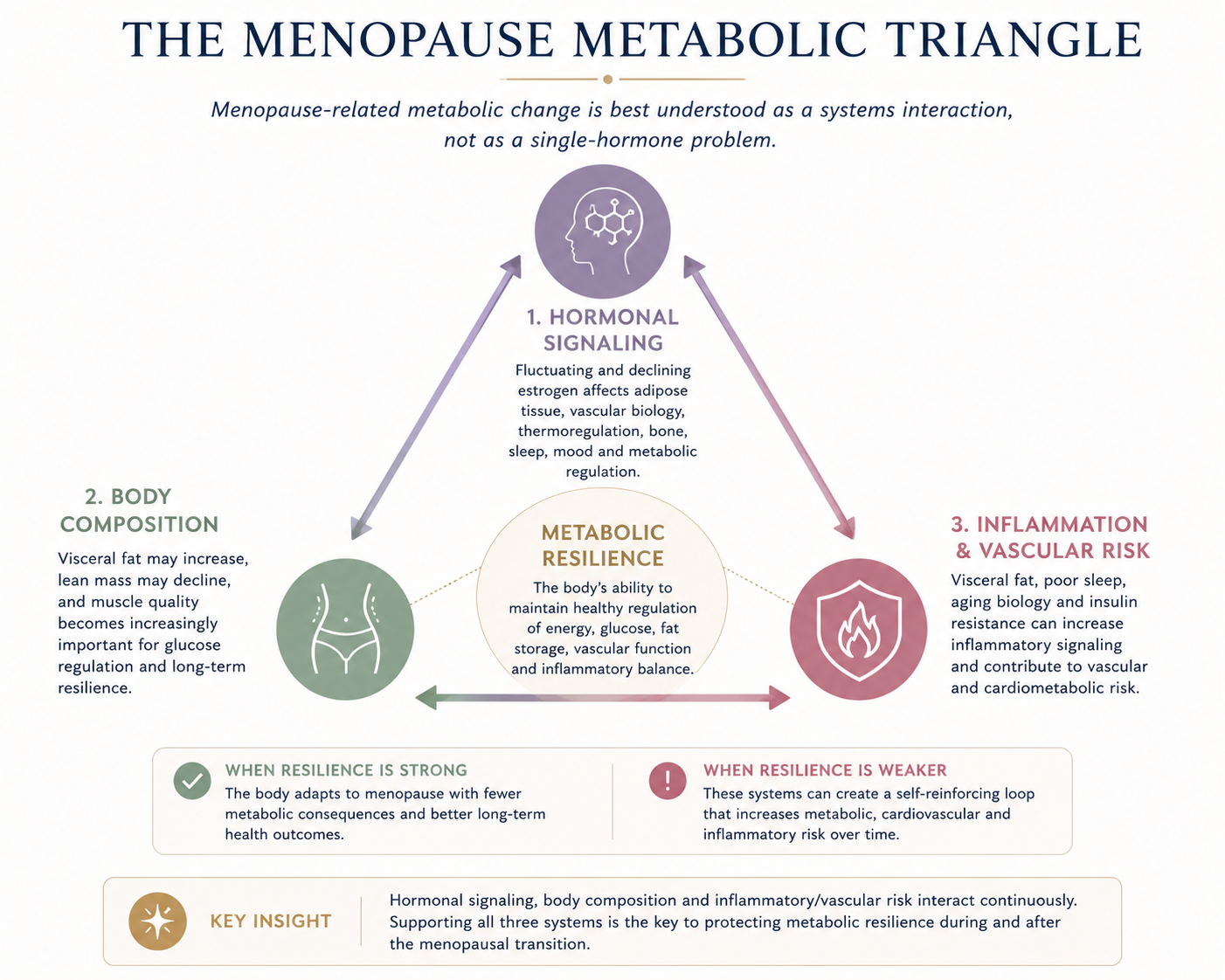
11. A systems model: the Menopause Metabolic Triangle
A useful way to understand the menopausal transition is through three interacting systems.
1. Hormonal signaling
Fluctuating and declining ovarian hormones affect thermoregulation, adipose tissue, vascular function, bone, sleep, mood and metabolic regulation.
2. Body composition
Visceral fat may increase, lean mass may decline, and muscle quality becomes increasingly important for glucose regulation and long-term resilience.
3. Inflammatory and vascular risk
Visceral fat, poor sleep, aging biology and insulin resistance can increase inflammatory signaling and contribute to vascular risk.
Together, these three systems influence metabolic resilience.
When resilience is strong, the body adapts to menopause with fewer long-term metabolic consequences. When resilience is weaker, menopause may become the period where risk begins to cluster.
12. Open questions in menopause science
Many important questions remain unresolved.
How much of cardiometabolic change is caused directly by ovarian aging, and how much is caused by chronological aging?
Why do some women experience rapid visceral fat gain while others do not?
Which biomarkers best identify women at high risk during the menopausal transition?
Can early resistance training, sleep intervention and metabolic monitoring prevent later insulin resistance and cardiovascular disease?
Which women benefit metabolically from hormone therapy, and which do not?
How should menopause care be personalized using inflammatory, metabolic, vascular, genetic or proteomic data?
Can artificial intelligence help detect risk patterns earlier by integrating symptoms, cycle history, laboratory markers, body composition and longitudinal trends?
These questions are exactly why menopause should be treated as an active research field, not only a symptom category.
Bottom line
Menopause is not just the end of reproductive cycling.
It is a biological transition that can reshape metabolism, body composition, vascular risk, inflammatory signaling, sleep and long-term health trajectory.
The most useful frame is not:
How do we treat menopause?
It is:
How do we protect metabolic resilience during and after the menopausal transition?
That shift turns menopause from a narrow hormonal topic into a prevention window.
For women’s health intelligence, this is one of the most important reframings: menopause is not only reproductive aging. It is metabolic remodeling.
Understanding that transition early may help prevent disease later.
Page summary
Menopause as a Metabolic Transition
Menopause is more than a hormonal milestone. It is a multi-year biological transition involving visceral fat, insulin resistance, lipid changes, vascular risk, inflammation, muscle, sleep and long-term metabolic resilience. This page introduces menopause as a prevention window and serves as the cornerstone article for the Menopause and Metabolic Change category.
Links
Next reading:
Why Visceral Fat Increases After Menopause
Menopause and Insulin Resistance
Menopause and Cardiovascular Risk
The Menopause Metabolic Assessment
Muscle, Mitochondria and Menopause
Hormone Therapy and Metabolic Health
References
1. The menopausal transition period and cardiovascular risk Nature Reviews Cardiology
This review explains the menopausal transition as a multi-year period associated with metabolic and cardiovascular changes. It is especially useful as a cornerstone reference because it discusses ovarian aging, chronological aging, cardiometabolic risk and the difficulty of separating these processes.
2. Menopause Transition and Cardiovascular Disease Risk: Implications for Timing of Early Prevention American Heart Association / Circulation
This scientific statement frames the menopausal transition as a period of accelerating cardiovascular risk. It supports the article’s prevention-window concept, emphasizing midlife as an important time for early risk monitoring and intervention.
3. The 2022 Hormone Therapy Position Statement of The North American Menopause Society The North American Menopause Society / Menopause
This position statement supports the balanced hormone therapy section. It states that hormone therapy remains the most effective treatment for vasomotor symptoms and genitourinary syndrome of menopause, while also emphasizing that risks vary depending on age, timing, dose, route, duration and individual risk factors.
4. Menopause transition and cardiovascular disease risk Maturitas
This review supports the idea that menopause is relevant to cardiovascular risk beyond general aging alone. It is useful for backing the article’s discussion of lipid changes, vascular risk and the importance of cardiovascular prevention after the menopausal transition.
5. Changes in abdominal subcutaneous adipose tissue phenotype and insulin sensitivity after menopause Scientific Reports / Nature Portfolio
This study supports the article’s section on body composition, central adiposity and insulin resistance. It describes menopause as being associated with redistribution of adipose tissue toward central fat accumulation, which is relevant to metabolic risk.
