
Why conception is not only about eggs, tubes and sperm
Endometriosis is often discussed as a cause of pelvic pain.
But for many women, the most important question is fertility.
Can endometriosis make it harder to become pregnant?
Can it affect implantation?
Does it reduce IVF success?
Does inflammation matter?
Should endometriosis be treated before trying to conceive?
Can anything be done to improve the reproductive environment?
The answer is not simple, because fertility is not one single function. It depends on ovulation, egg quality, sperm function, fallopian tube movement, pelvic anatomy, inflammation, immune signaling, endometrial receptivity, implantation, embryo quality and timing.
Endometriosis can interact with several of these systems.
This is why it is more useful to think in terms of the implantation environment.
Not only:
Can the egg be fertilized?
But also:
Is the reproductive environment supportive enough for fertilization, implantation and early pregnancy?
Endometriosis and infertility: what is established
Endometriosis is associated with infertility, but the effect varies widely between women.
Some women with endometriosis conceive naturally. Others need medical assistance, surgery, ovulation support or IVF. Some have mild-looking disease but significant fertility problems. Others have extensive disease and still conceive.
ESHRE describes endometriosis care as including diagnosis and treatment of both pain and infertility, including medically assisted reproduction when relevant.
The important point is that endometriosis can affect fertility through multiple pathways:
- pelvic inflammation
- adhesions and distorted anatomy
- impaired tubal function
- ovarian endometriomas
- reduced ovarian reserve in some cases
- altered egg or follicular environment
- inflammatory changes around sperm, egg or embryo
- altered endometrial receptivity
- progesterone resistance
- implantation dysfunction
- coexistence with adenomyosis or other uterine factors
This is why endometriosis-related infertility should not be explained by one mechanism alone.
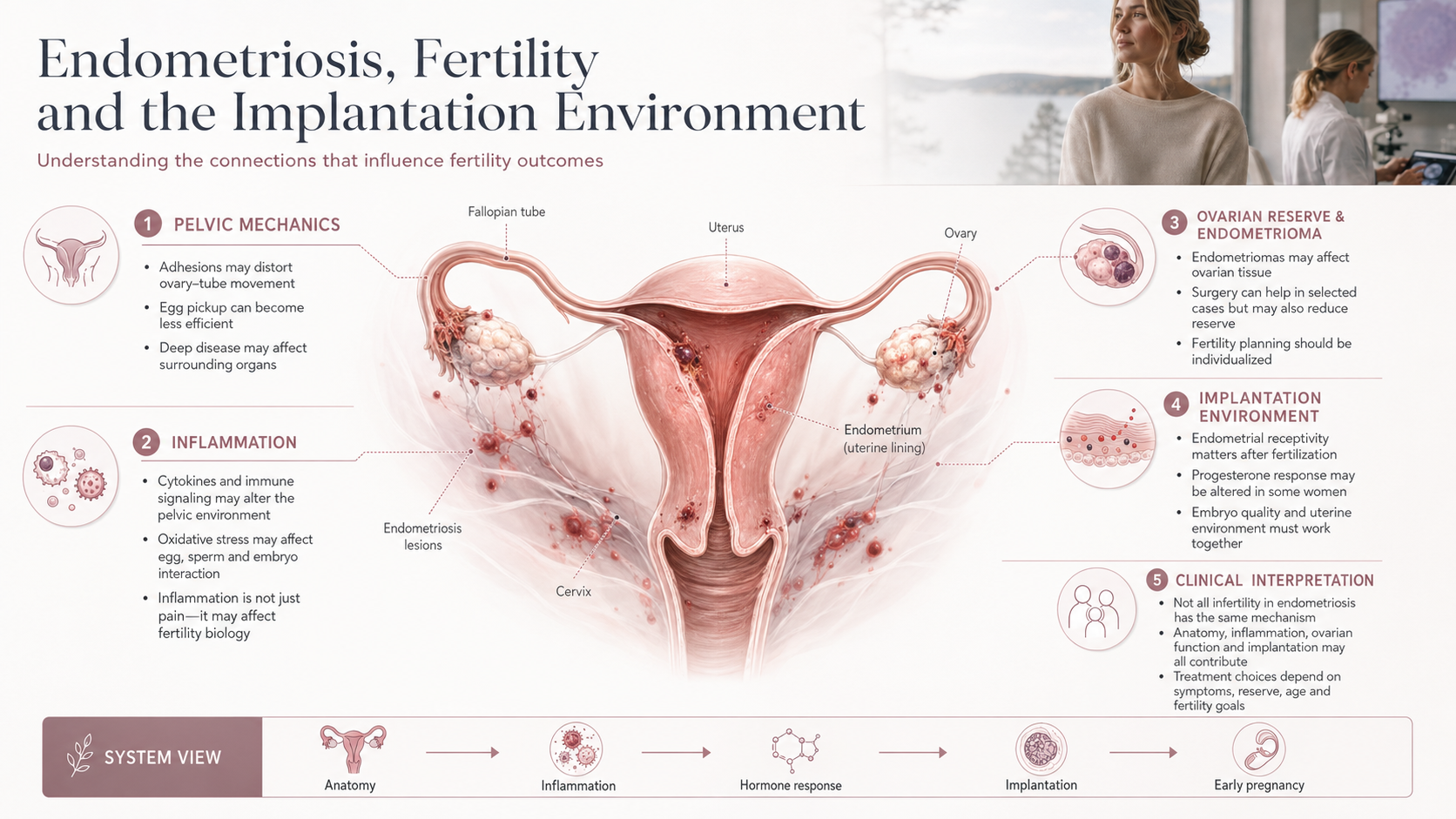
The mechanical side: anatomy, adhesions and organ movement
The most visible fertility mechanism is mechanical.
Endometriosis can cause inflammation, fibrosis and adhesions. Adhesions may restrict how pelvic organs move in relation to each other.
This can affect fertility if adhesions interfere with:
- the ovary releasing an egg normally
- the fallopian tube picking up the egg
- movement of the egg through the tube
- normal relationship between ovary and tube
- pelvic anatomy around the uterus and ovaries
Deep endometriosis and ovarian endometriomas can also alter anatomy and complicate fertility planning.
However, mechanical distortion is not the whole story.
Some women with minimal visible disease have infertility. This suggests that inflammation, ovarian environment and implantation biology may also matter.
The inflammatory side: a hostile reproductive environment
Endometriosis is an inflammatory disease.
Inflammation in the pelvis may affect fertility by changing the environment around the ovary, tube, sperm, egg and embryo.
Inflammatory mediators, immune cells, oxidative stress and altered cytokine signaling may influence:
- follicle development
- egg quality
- sperm function
- fertilization
- embryo development
- tubal function
- implantation
- early pregnancy signaling
This does not mean inflammation explains every case of infertility.
But it does mean that fertility in endometriosis is not only a plumbing problem.
The reproductive environment may be biologically altered even when anatomy looks acceptable.
Ovarian endometriomas and ovarian reserve
Ovarian endometriomas are endometriosis-related cysts in the ovary.
They matter for fertility because they may be associated with:
- reduced ovarian reserve
- inflammation in ovarian tissue
- altered response to stimulation
- surgical decision complexity
- risk of losing healthy ovarian tissue during cyst surgery
- possible effects on egg retrieval access in IVF
This creates a difficult balance.
Removing an endometrioma may help pain or make fertility treatment easier in some situations, but surgery can also reduce ovarian reserve if healthy ovarian tissue is damaged.
This is why decisions about endometrioma surgery before fertility treatment should be individualized.
The question is not simply:
Should it be removed?
The better question is:
What is the size, location, symptom burden, ovarian reserve, IVF plan, surgical risk and fertility timeline?
Endometrial receptivity: the uterus side of fertility
Fertility does not end with the egg.
The embryo must implant into a receptive endometrium.
In endometriosis, the eutopic endometrium — the lining inside the uterus — may also show altered molecular and immune behavior, even though the visible lesions are outside the uterus.
Research describes mechanisms in endometriosis-associated infertility that include hormonal dysregulation, inflammation, altered apoptosis, neuroangiogenesis, oxidative stress and endometrial changes.
This raises important questions:
Is the endometrium receptive at the right time?
Is progesterone signaling normal?
Is inflammation interfering with implantation?
Are immune and vascular signals balanced?
Is the embryo entering a stable environment?
These questions are especially relevant in IVF, where embryo quality may be known, but implantation still fails.
Progesterone resistance and implantation
Progesterone is essential for preparing the endometrium for implantation.
After ovulation, progesterone helps transform the endometrium into a secretory, receptive and pregnancy-supportive tissue. If pregnancy occurs, progesterone supports decidualization and early pregnancy maintenance.
In endometriosis, progesterone responsiveness may be altered. This is often called progesterone resistance.
A review of progesterone resistance in endometriosis describes increasing evidence for loss of progesterone signaling, with possible contributors including abnormal progesterone receptor signaling, chronic inflammation, aberrant gene expression and epigenetic changes.
This may matter for fertility because impaired progesterone response could affect:
- endometrial receptivity
- decidualization
- immune tolerance
- inflammatory control
- implantation stability
- early pregnancy support
This does not mean every woman with endometriosis has clinically important progesterone resistance.
But it is one of the most important biological concepts connecting endometriosis to implantation.
IVF outcomes: why the evidence is complex
IVF can bypass some mechanical problems caused by endometriosis, especially tubal pickup or pelvic adhesions.
But IVF does not automatically bypass every endometriosis-related issue.
Potential remaining factors include:
- ovarian reserve
- egg quality
- stimulation response
- endometrioma effects
- inflammation
- uterine receptivity
- adenomyosis overlap
- embryo transfer environment
- progesterone response
- underlying infertility factors
A 2024 systematic review and meta-analysis evaluated the impact of endometriosis on IVF outcomes, including live birth, clinical pregnancy, fertilization and implantation rates, showing that IVF outcome research remains an active and complex field.
The honest interpretation is:
Endometriosis can influence IVF outcomes, but the effect depends on disease type, ovarian reserve, age, embryo quality, adenomyosis, prior surgery, protocol, and whether the main problem is ovarian, anatomical, inflammatory or endometrial.
This is why one IVF strategy does not fit all patients with endometriosis.
Should endometriosis be treated before trying to conceive?
This depends on the situation.
Factors that matter include:
- age
- duration of infertility
- pain severity
- suspected disease type
- ovarian reserve
- presence and size of endometrioma
- tubal status
- partner sperm factors
- previous surgery
- previous IVF attempts
- suspicion of adenomyosis
- urgency of fertility treatment
- access to specialist surgery
- personal priorities
NICE guidance includes diagnosis and management of endometriosis where fertility is a priority and emphasizes access to specialist services, imaging, pain management and fertility services when appropriate.
In some cases, surgery may improve fertility or pain. In others, moving directly to IVF may be more appropriate. In some women, hormonal suppression may reduce symptoms but is not compatible with trying to conceive during treatment.
The key is individualized planning.
Can the implantation environment be improved?
This is one of the most important questions.
Some factors may be modifiable. Others may not be fully controllable.
Potential strategies may include:
Specialist diagnosis and mapping
Understanding whether disease is superficial, ovarian, deep, bowel-related, bladder-related or associated with adenomyosis can guide decisions.
Treating significant pain or deep disease
In selected cases, treatment of deep disease or severe symptoms may improve quality of life and clarify fertility planning.
Protecting ovarian reserve
Endometrioma surgery should be considered carefully, especially if ovarian reserve is already reduced.
Optimizing IVF planning
Protocol choice, timing, endometrioma management, embryo strategy and transfer planning may need individualization.
Managing inflammation and general health
There is no proven universal anti-inflammatory protocol for endometriosis fertility. But reducing modifiable inflammatory burden, addressing metabolic health, correcting deficiencies and supporting sleep, stress physiology and gut symptoms may help overall resilience.
Considering adenomyosis
Adenomyosis can coexist with endometriosis and may affect implantation or pregnancy outcomes. It should be considered when symptoms or imaging suggest it.
Avoiding over-treatment
Not every finding requires surgery. Not every patient benefits from suppression before IVF. Not every supplement improves outcomes.
The best fertility strategy is not the most aggressive one.
It is the one that matches the mechanism most likely to matter in that patient.
What patients often want to know
Women with endometriosis and infertility often ask very intelligent questions:
Is my problem egg quality, implantation or inflammation?
Does my endometrioma reduce my chances?
Would surgery help or harm my ovarian reserve?
Should I do IVF first or surgery first?
Could progesterone resistance affect transfer success?
Does inflammation make miscarriage more likely?
Should I suppress disease before embryo transfer?
Could adenomyosis be part of the problem?
What can I actually influence?
These questions are valid.
They should not be dismissed with “just try IVF” or “just relax.”
Endometriosis fertility care needs mechanism-based thinking.
What remains uncertain
Several important questions remain open:
Which biomarkers can reliably identify inflammation-related infertility?
Which women benefit from surgery before IVF?
When does endometrioma removal help fertility, and when does it reduce ovarian reserve too much?
How should progesterone resistance be measured clinically?
Which patients benefit from pre-treatment before embryo transfer?
How much does endometriosis affect implantation compared with embryo quality?
How should adenomyosis be integrated into fertility planning?
Can multi-omics or AI-supported models improve individualized prediction?
These are research questions, not settled answers.
The High Coast view: fertility as a systems problem
Endometriosis-related fertility should be understood as a systems problem.
It may involve:
Pelvic anatomy
↓
Ovarian reserve
↓
Inflammation
↓
Hormone response
↓
Endometrial receptivity
↓
Embryo implantation
↓
Early pregnancy stability
This does not mean every woman has dysfunction at every level.
It means that proper interpretation requires more than one lens.
For some women, the main barrier may be anatomy.
For others, ovarian reserve.
For others, implantation biology.
For others, inflammation or adenomyosis.
For many, several factors overlap.
Key message
Endometriosis can affect fertility through more than one pathway.
It may alter pelvic anatomy, ovarian function, inflammation, hormone response, endometrial receptivity, implantation and IVF outcomes.
The implantation environment is not a vague concept. It is the biological context in which embryo, endometrium, immune signaling, progesterone response and vascular remodeling must work together.
The goal is not to blame endometriosis for every fertility problem.
The goal is to understand which mechanisms may matter, what can be measured, what can be treated, and what remains uncertain.
References and Resource
- Endometriosis guideline ESHRE — European Society of Human Reproduction and Embryology
Best-practice guideline covering endometriosis diagnosis, pain treatment, infertility and medically assisted reproduction. - Endometriosis: diagnosis and management NICE — National Institute for Health and Care Excellence
Guideline covering endometriosis diagnosis and management, including when fertility is a priority and access to specialist services - Endometriosis-associated infertility: Multi-omics insights into mechanisms, therapeutics, and assisted reproduction Frontiers in Endocrinology / NIH PMC
Review of mechanisms in endometriosis-associated infertility, including hormonal dysregulation, inflammation, oxidative stress and endometrial changes - Progesterone Resistance in Endometriosis: Current Evidence and Putative Mechanisms International Journal of Molecular Sciences / MDPI
Review of progesterone resistance mechanisms in endometriosis and their relevance to inflammation and reproductive function. - The Effect of Endometriosis on In Vitro Fertilization Outcomes: A Systematic Review and Meta-Analysis Healthcare / MDPI
Systematic review and meta-analysis evaluating the impact of endometriosis on IVF outcomes such as live birth, clinical pregnancy, fertilization and implantation.
