Why the mid-pregnancy anatomy scan can change how a hematoma is understood
A pregnancy hematoma can mean different things depending on when it is found.
A small hematoma detected in early pregnancy is not the same situation as a hematoma that is still present, newly discovered or more clearly described around week 18–22.
This period is important because it is usually when the detailed mid-pregnancy ultrasound is performed. At this stage, the fetus is larger, the placenta is easier to assess, the cervix may be evaluated, and the relationship between the hematoma, placenta, membranes and uterine wall can often be described more clearly.
For many women, this is also the stage when a vague early finding becomes more concrete.
The question is no longer only:
Is there a hematoma?
The more useful questions are:
Where is it?
How large is it?
Is it close to the placenta?
Is it behind the placenta or near the edge?
Is it changing?
Is there ongoing bleeding?
Is the cervix reassuring?
Is fetal growth appropriate?
Is the placenta otherwise normal?
Around week 18–22, anatomy matters more than ever.
Why week 18–22 is a special window
The mid-pregnancy ultrasound, often called the anatomy scan, is commonly performed around 18–22 weeks.
This scan is not only about looking at the baby’s organs. It also gives important information about the pregnancy environment.
Depending on local practice and clinical indication, the scan may assess:
- fetal anatomy
- fetal growth and measurements
- fetal heartbeat and movement
- amniotic fluid
- placental location
- placental appearance
- cord insertion
- cervix and lower uterus
- uterus and adnexa
- visible bleeding collections or hematomas
This makes week 18–22 an important time to understand a hematoma in relation to the full pregnancy anatomy.
A hematoma that was earlier described simply as “subchorionic” may now be interpreted more precisely in relation to the placenta, uterine wall and membranes.
That precision can matter.
The fetus is larger — and the tissue relationships are clearer
At 18–22 weeks, the baby is large enough that the uterus, placenta and membranes have a more developed spatial relationship.
The placenta is more established. The amniotic cavity is larger. The uterine wall has expanded. The cervix and lower uterine segment may be more relevant if bleeding has occurred.
This means an ultrasound can often give a clearer picture of where a blood collection sits.
For example, a hematoma may appear:
- along the membranes
- near the placental edge
- under or beside the placenta
- behind the placenta
- near the cervix
- in relation to a low-lying placenta
- as an older, organized collection rather than fresh bleeding
This is why a hematoma around week 18–22 should not be interpreted only by its name. Its anatomical relationship to the placenta and uterine wall matters.
Why placental relationship matters
The placenta is the central exchange organ between mother and fetus. It anchors into the uterine wall and supports oxygen and nutrient transfer.
A hematoma near the membranes may have one kind of meaning. A hematoma at the placental edge may have another. A hematoma behind the placenta can be more concerning, especially if it is associated with pain, uterine tenderness, contractions or ongoing bleeding.
The important question is whether the hematoma appears to involve the placental attachment area.
This does not mean that every hematoma near the placenta leads to a poor outcome. Many pregnancies continue normally.
But it does mean the finding deserves careful interpretation.
In clinical thinking, the placenta is not just a background structure. It is part of the risk context.
Subchorionic, marginal and retroplacental: why the words matter
A hematoma around week 18–22 may be described using different terms.
Subchorionic hematoma
A subchorionic hematoma is usually described as blood between the chorion or membranes and the uterine lining. This term is often used earlier in pregnancy, but subchorionic collections can also remain visible later.
At week 18–22, the key question is how close the collection is to the placenta and whether it is stable, shrinking or associated with symptoms.
Marginal hematoma
A marginal hematoma is located near the edge of the placenta.
This location can be important because it sits at the boundary between placental tissue and surrounding membranes or uterine wall. Bleeding at the placental edge may produce intermittent vaginal bleeding or older brown discharge.
Its meaning depends on size, persistence, symptoms and placental assessment.
Retroplacental hematoma
A retroplacental hematoma is located behind the placenta, between the placenta and uterine wall.
This can be more clinically significant because it may suggest bleeding near the placental attachment site. It should be interpreted carefully, especially if there is pain, uterine tenderness, contractions, heavy bleeding or fetal concerns.
The distinction between these locations is one reason why the anatomy scan period can be so useful.
What patients often notice around this time
Some women already know they have a hematoma from earlier scans.
Others first learn about it at the anatomy scan.
Some may have had bleeding weeks earlier and are surprised that the hematoma is still visible. Others may have brown discharge or spotting and wonder whether it represents old blood or new bleeding.
Common experiences include:
- old hematoma still visible
- hematoma smaller but not gone
- change in shape or ultrasound appearance
- intermittent brown discharge
- recurrent spotting
- anxiety before or after the anatomy scan
- confusion about whether the finding is “important”
These concerns are reasonable.
A hematoma can be both common enough to be monitored conservatively and important enough to deserve proper explanation.
Why persistence does not always mean active bleeding
A hematoma visible at week 18–22 does not necessarily mean there is ongoing active bleeding.
Old blood can remain visible for weeks. It may organize, change texture and slowly resorb. Some blood may leave through the cervix as brown discharge.
This means that persistence on ultrasound can sometimes reflect slow clearance rather than new bleeding.
However, this should not be assumed automatically. New symptoms, fresh bleeding, pain or contractions may change the interpretation.
The key is trend and context:
Is it shrinking?
Is it stable?
Is it growing?
Is the blood older in appearance?
Are symptoms improving or worsening?
Is the placenta reassuring?
Is fetal growth appropriate?
These questions are more useful than asking only whether the hematoma is still visible.
Why symptoms and ultrasound must be interpreted together
The same ultrasound finding can feel very different depending on symptoms.
A small stable hematoma without bleeding may be interpreted differently from a larger hematoma with recurrent red bleeding and pain.
Important clinical context includes:
- amount of bleeding
- color and pattern of bleeding
- pain or cramping
- contractions
- uterine tenderness
- cervical findings
- placental location
- fetal movement later in pregnancy
- fetal growth
- previous miscarriage
- IVF history
- endometriosis or inflammatory history
- medication history, including anticoagulants if relevant
Patients often want one clear answer from the ultrasound report. But pregnancy hematoma interpretation is usually not one-variable medicine.
It is pattern interpretation.
Why week 18–22 can be emotionally difficult
The anatomy scan is often described as a milestone.
For women with previous loss, IVF history, bleeding episodes or hematoma, it can also be a point of intense anxiety.
This is the time when many patients expect reassurance. But if a hematoma is still visible, or if the report uses unclear language, the scan can instead create more uncertainty.
Patients may be told:
“It is probably old blood.”
“We will monitor it.”
“It is not unusual.”
“Come back if bleeding increases.”
These statements may be clinically reasonable, but they may not be enough.
A well-informed patient may need to understand:
- what kind of hematoma it is
- where it is located
- whether it is near the placenta
- how it compares with earlier scans
- what symptoms should trigger contact
- whether follow-up is planned
- whether fetal growth or placenta needs later reassessment
Good explanation matters because uncertainty itself is a burden.
What could be documented more clearly
A useful hematoma description around week 18–22 may include:
- location
- size in measurements
- relationship to placenta
- relationship to membranes
- relationship to cervix or lower uterus if relevant
- whether it appears fresh or organized
- whether there is comparison with previous scans
- placental location
- cord insertion if assessed
- amniotic fluid
- fetal growth and anatomy findings
- follow-up plan
Not every report will include all of this. But these are the kinds of details that help turn a vague finding into structured understanding.
This is where Pregnancy Intelligence can add value: not by replacing clinical care, but by helping organize the questions and patterns that matter.
What is known — and what remains uncertain
It is established that hematomas can be seen on ultrasound and that location, size, symptoms and gestational age matter for interpretation.
It is also established that the 18–22 week scan is an important time for fetal anatomy and pregnancy structure assessment.
What is less certain is exactly how different hematoma types behave in different patients.
Research on subchorionic hematoma is mixed. Some studies associate hematoma with increased risk of miscarriage, preterm birth, placental abruption or other outcomes, while other studies find weaker or no associations depending on population and study design.
This does not mean the finding should be ignored.
It means it should be interpreted carefully, without panic and without false reassurance.
Research perspective: why this window is interesting
Week 18–22 is interesting not only clinically, but also scientifically.
At this stage, several important data points can be connected:
- hematoma location
- placental position
- placental interface
- cervical assessment
- fetal anatomy
- fetal growth
- bleeding history
- IVF or miscarriage history
- inflammatory conditions such as endometriosis
- symptom trends
- future pregnancy outcomes
This creates an opportunity for better models.
Research questions include:
Can hematoma location at 18–22 weeks predict persistence?
Does placental-edge bleeding behave differently from membrane bleeding?
Can ultrasound appearance distinguish old organized blood from higher-risk patterns?
Do inflammation-related histories change risk patterns?
Can symptom tracking improve interpretation between scans?
Can AI-supported pattern recognition help structure follow-up without replacing clinicians?
These are open questions, not established answers.
When to seek medical care
Any bleeding during pregnancy should be discussed with a healthcare provider.
Urgent assessment is especially important if there is:
- heavy bleeding
- severe abdominal pain
- dizziness or fainting
- contractions
- fluid leakage
- fever
- uterine tenderness
- reduced fetal movement later in pregnancy
- a sudden change in symptoms
This article is educational and does not replace medical care.
Key message
Around week 18–22, a pregnancy hematoma should be understood anatomically.
The important question is not only whether a hematoma exists.
The important question is where it sits, how it relates to the placenta and uterine wall, whether it is changing, and how the ultrasound finding fits with symptoms and pregnancy history.
This is why timing matters.
At the anatomy scan stage, a hematoma becomes part of a larger pregnancy map.
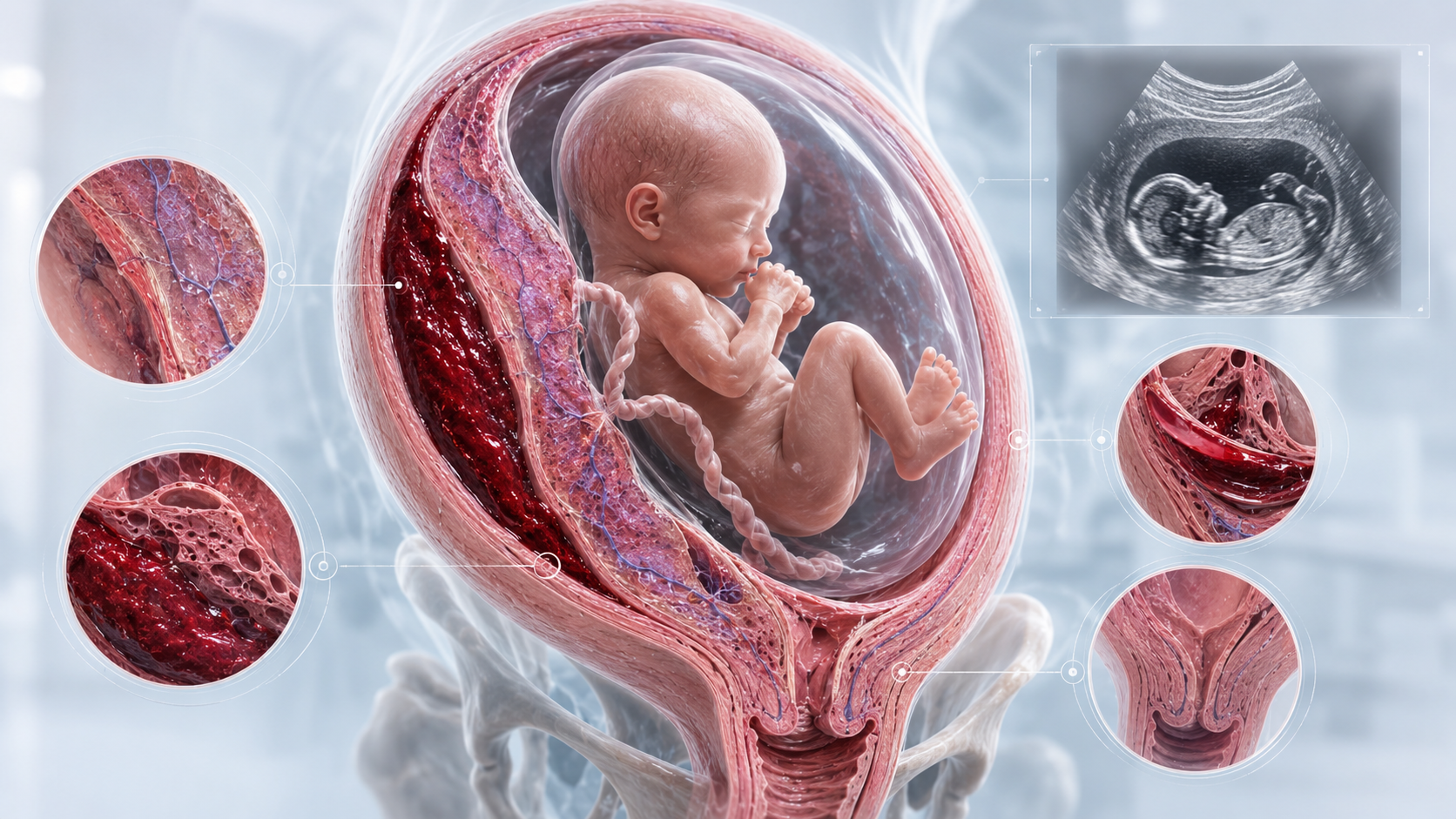
Figure: Pregnancy hematoma around week 18–22.
The main image shows a cross-section of the pregnant uterus with the fetus inside the amniotic sac. The placenta is shown along the uterine wall, and the hematoma is visible as a dark red blood collection close to the placental and uterine interface.
The surrounding detail images highlight why anatomical location matters. The upper left image shows the tissue plane between the uterine wall and pregnancy membranes. The lower left image shows a darker, more organized blood collection. The upper right ultrasound-style image represents how the pregnancy may be assessed during the mid-pregnancy scan. The middle right image focuses on the placental or membrane interface where blood may collect. The lower right image shows the lower uterus and cervix, which are relevant when bleeding or drainage is being evaluated.
The image is intended to show that a hematoma around week 18–22 should be interpreted as part of the full pregnancy anatomy: fetus, amniotic sac, placenta, uterine wall, cervix and the exact position of the blood collection. It is an educational illustration, not a diagnostic ultrasound image.
References and Resources
- Ultrasound Exams ACOG — American College of Obstetricians and Gynecologists
Supports that a standard pregnancy ultrasound is usually performed at 18–22 weeks and may be used to assess fetal development and pregnancy findings.
- ISUOG Practice Guidelines: Performance of the routine mid-trimester fetal ultrasound scan ISUOG — International Society of Ultrasound in Obstetrics and Gynecology
Supports the 18–22 week mid-trimester scan window and the importance of structured fetal and pregnancy assessment. - Society for Maternal-Fetal Medicine Consult Series #60: Management of Pregnancies Resulting from IVF SMFM — Society for Maternal-Fetal Medicine
Relevant for IVF pregnancy context and careful assessment of placental location, placental shape and cord insertion at the fetal anatomy ultrasound. - Subchorionic Hemorrhage in the Second and Third Trimesters of Pregnancy: A Review Obstetrical & Gynecological Survey
Review focused on SCH in later pregnancy, including diagnosis, outcomes and management challenges in second and third trimester cases. - Subchorionic hematoma: Research status and pathogenesis Medicine International / Spandidos Publication Overview of SCH definition, unclear pathogenesis, outcome uncertainty and the need for further research.
