
Supportive biology, clinical use and evidence limits
Progesterone is one of the most important hormones in pregnancy.
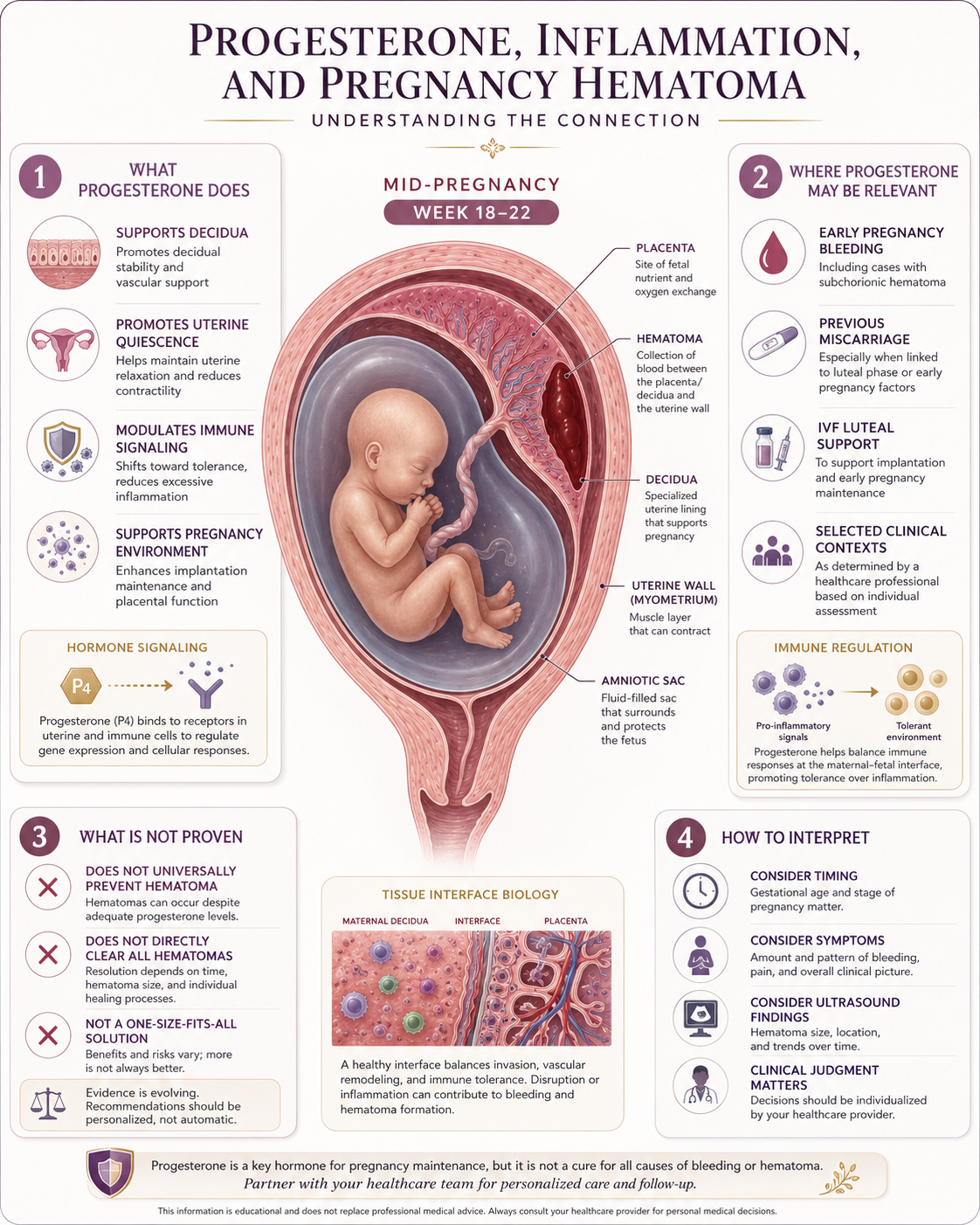
It supports the uterine lining, helps maintain early pregnancy, contributes to immune tolerance at the maternal-fetal interface and helps keep the uterus in a pregnancy-supportive state.
Because of this, many women naturally ask whether progesterone could help when a pregnancy hematoma is found.
The answer is nuanced.
Progesterone is biologically relevant to pregnancy tissue stability, immune regulation and early pregnancy support. In selected situations, progesterone may be used clinically, especially in early pregnancy bleeding with a history of miscarriage, depending on local guidelines and individual assessment.
But progesterone should not be described as a proven treatment that clears or prevents all pregnancy hematomas.
That distinction is important.
Progesterone may support the pregnancy environment.
It may be clinically appropriate in some contexts.
It is not a universal hematoma treatment.
Why progesterone matters in pregnancy
Progesterone helps prepare and maintain the uterine environment for pregnancy.
Before pregnancy, progesterone helps transform the endometrium into a receptive lining. After implantation, progesterone supports decidualization, the process by which the uterine lining becomes specialized pregnancy tissue.
During pregnancy, progesterone is involved in:
- decidual function
- pregnancy maintenance
- immune tolerance
- reduced uterine contractility
- communication at the maternal-fetal interface
- regulation of inflammatory responses
- support of early placental development
This is why progesterone is often called a pregnancy-supporting hormone.
But “important” does not automatically mean “treatment for every complication.”
Progesterone and the maternal-fetal interface
The maternal-fetal interface is the region where maternal tissue, decidua, placenta and fetal-derived membranes interact.
This interface must allow pregnancy tissue to attach, grow and communicate with maternal circulation while avoiding excessive immune activation.
Progesterone is one of the hormones involved in this balance.
It can influence immune cells, inflammatory signaling, decidual cells and the local pregnancy environment. Research describes progesterone as having broad immunomodulatory roles in the decidua, placenta, myometrium and maternal circulation.
This makes progesterone highly relevant when discussing inflammation and pregnancy.
However, relevance is not the same as direct proof.
A hematoma is a visible blood collection. It may involve local bleeding, tissue separation, vascular fragility, placental-edge changes or other mechanisms. Progesterone may influence some background conditions, but it does not automatically explain or reverse the hematoma itself.
Why progesterone is discussed after bleeding
Progesterone is often discussed in early pregnancy bleeding because low progesterone levels have been associated with threatened miscarriage and early pregnancy loss.
Some guidelines recommend vaginal micronized progesterone for women with early pregnancy bleeding who have had previous miscarriage, after an intrauterine pregnancy is confirmed.
This is not the same as saying progesterone treats the hematoma.
The clinical logic is usually broader:
- support the pregnancy in selected higher-risk early bleeding situations
- reduce miscarriage risk in certain patient groups
- support the endometrial/decidual environment
- avoid assuming all bleeding has the same cause
If a woman has bleeding and a hematoma, progesterone may be discussed because of the bleeding and pregnancy history, not necessarily because progesterone directly clears the hematoma.
This distinction should be made clear.
Progesterone and hematoma: what is not proven
It would be too strong to say:
Progesterone prevents pregnancy hematomas.
Progesterone clears pregnancy hematomas.
Progesterone closes the bleeding site.
Progesterone solves inflammation behind all hematomas.
The evidence does not support such broad statements.
A more accurate statement is:
Progesterone has important roles in pregnancy maintenance and immune regulation. In selected clinical contexts, especially early pregnancy bleeding with previous miscarriage, progesterone may be considered or recommended depending on guidelines. But its role as a specific treatment for pregnancy hematoma is uncertain.
This protects both scientific accuracy and patient trust.
Could progesterone calm inflammation?
Progesterone can influence immune and inflammatory pathways in pregnancy.
It may help support a more pregnancy-tolerant immune environment and reduce certain inflammatory reactions. This is part of its biological importance.
But the phrase “calm inflammation” should be used carefully.
Inflammation in pregnancy is not always abnormal. Some immune activity is necessary for implantation, placental development and tissue remodeling. The problem is not inflammation itself, but poorly regulated or excessive inflammation in the wrong context.
So a careful interpretation is:
Progesterone is involved in immune regulation at the pregnancy interface. It may help support a pregnancy-tolerant environment. Whether this directly reduces hematoma formation or speeds hematoma clearance is not established.
This is the right balance.
Why timing matters
Progesterone biology changes over pregnancy.
In early pregnancy, progesterone is initially supported by the corpus luteum. Later, the placenta takes over progesterone production.
This is one reason progesterone treatment discussions are often focused on early pregnancy.
A hematoma found around week 18–22 is a different situation from bleeding at six or seven weeks.
By mid-pregnancy, the placenta is established, the anatomy is clearer, and hematoma interpretation depends more strongly on location, placental relationship, size, symptoms and trend over time.
Progesterone may still be relevant in some clinical situations, but it should not be assumed to be the central answer for every second-trimester hematoma.
IVF and progesterone support
Progesterone is commonly used in IVF and frozen embryo transfer cycles as luteal phase or pregnancy support.
This can make hematoma interpretation confusing.
If a hematoma appears during an IVF pregnancy, the patient may wonder:
Was my progesterone too low?
Was the route of progesterone wrong?
Should progesterone be increased?
Did stopping progesterone cause bleeding?
Is the hematoma a sign of inadequate support?
These are understandable questions, but they cannot be answered generally.
IVF pregnancies differ in protocol, embryo transfer type, hormone support, infertility diagnosis, endometriosis history, maternal age and monitoring intensity.
A hematoma in an IVF pregnancy should not automatically be interpreted as progesterone failure.
Progesterone status may be one part of the context, but hematoma formation is likely multifactorial in many cases.
Progesterone, endometriosis and decidual function
Progesterone is also interesting in endometriosis research because endometriosis has been associated in some studies with altered progesterone responsiveness.
This may affect endometrial receptivity, inflammatory signaling and decidual function.
For women with endometriosis, this raises a reasonable research question:
Could altered progesterone signaling influence the pregnancy tissue interface and bleeding susceptibility?
This is biologically plausible.
But again, it is not the same as proven clinical causation.
A responsible statement is:
In women with endometriosis, progesterone biology may be relevant to implantation and decidual function. Whether altered progesterone response directly contributes to pregnancy hematoma remains uncertain.
What progesterone can and cannot do
Progesterone may help support a pregnancy environment in selected situations.
It may be relevant to:
- early pregnancy support
- threatened miscarriage in certain groups
- luteal support after IVF
- decidual function
- immune regulation
- uterine quiescence
But progesterone cannot be assumed to:
- remove a hematoma
- drain old blood
- reverse every bleeding episode
- repair every placental-interface injury
- eliminate all miscarriage risk
- replace ultrasound follow-up
- replace clinical assessment
This is not a negative view of progesterone.
It is a realistic one.
The problem with “one-treatment” thinking
Pregnancy hematoma is often multifactorial.
It may involve:
- small-vessel bleeding
- membrane separation
- placental-edge bleeding
- uterine or decidual tissue vulnerability
- inflammation
- IVF or implantation context
- coagulation factors
- mechanical tissue relationships
- chance
If the cause is multifactorial, one intervention is unlikely to be universally effective.
Progesterone may be part of care in some cases. But hematoma monitoring still depends on anatomy, symptoms, ultrasound trend and pregnancy context.
The question should not be:
Does progesterone fix hematoma?
A better question is:
In which patient groups, at which gestational ages, and with which bleeding patterns might progesterone support improve pregnancy outcomes?
That is a research question worth asking.
What should patients ask their clinician?
Patients may want to ask:
Is progesterone relevant in my specific case?
Is my pregnancy in the gestational window where progesterone is usually considered?
Is the recommendation based on bleeding, previous miscarriage, IVF protocol or something else?
Is the hematoma itself the reason, or my broader risk history?
How long would progesterone be used if recommended?
What are the expected benefits and limits?
What follow-up is planned regardless of progesterone?
What symptoms should prompt urgent assessment?
These questions are reasonable and mature.
They help move the conversation from “Should I take progesterone?” to “What is the clinical reasoning in my situation?”
Safety and medical supervision
Progesterone should be used according to medical guidance.
Even when a treatment is commonly used, the indication, dose, route and duration should be decided by a qualified clinician with knowledge of the pregnancy history and current findings.
This is especially important in pregnancies involving IVF, previous miscarriage, bleeding, hematoma, multiple medications or other medical risk factors.
This article is educational and does not recommend starting, stopping or changing progesterone without medical advice.
Key message
Progesterone is biologically important in pregnancy and has real roles in decidual function, immune regulation and pregnancy support.
In selected clinical contexts, especially early pregnancy bleeding with previous miscarriage, progesterone may be used or recommended.
But progesterone is not proven as a universal treatment for pregnancy hematoma.
The honest position is this:
Progesterone may support the pregnancy environment in some situations, but hematoma formation and resolution are complex. The role of progesterone should be interpreted through timing, symptoms, pregnancy history, ultrasound findings and clinical guidance — not as a one-size-fits-all solution.
References and Resources
- Ectopic pregnancy and miscarriage: diagnosis and initial management — Evidence review C: Progestogens for preventing miscarriage NICE — National Institute for Health and Care Excellence
Evidence review supporting the role of progesterone in selected early pregnancy bleeding contexts, especially with previous miscarriage - The Effects of Progesterone on Immune Cellular Function at the Maternal-Fetal Interface and Maternal Circulation Journal of Steroid Biochemistry and Molecular Biology / NIH PMC
Review of progesterone’s immunomodulatory functions in the decidua, placenta, myometrium and maternal circulation - Progesterone: A Unique Hormone with Immunomodulatory Roles in Pregnancy International Journal of Molecular Sciences / MDPI
Review describing progesterone’s pregnancy roles and its ability to regulate immune and inflammatory responses - Micronized vaginal progesterone to prevent miscarriage: a critical evaluation of randomized evidence American Journal of Obstetrics & Gynecology
Review and critical evaluation of randomized evidence on progesterone for miscarriage prevention - Subchorionic hematoma: Research status and pathogenesis Medicine International / Spandidos Publications
Background review on SCH definition, pathogenesis uncertainty, treatment limitations and mixed evidence.
