
Why progesterone biology may need better measurement, timing and spatial thinking
Progesterone is often measured as a blood value.
That is understandable. Blood tests are accessible, standardized and clinically useful in many situations. In fertility care and pregnancy support, serum progesterone can provide important information about whether progesterone exposure may be too low, too high or mistimed.
But serum progesterone is not the whole story.
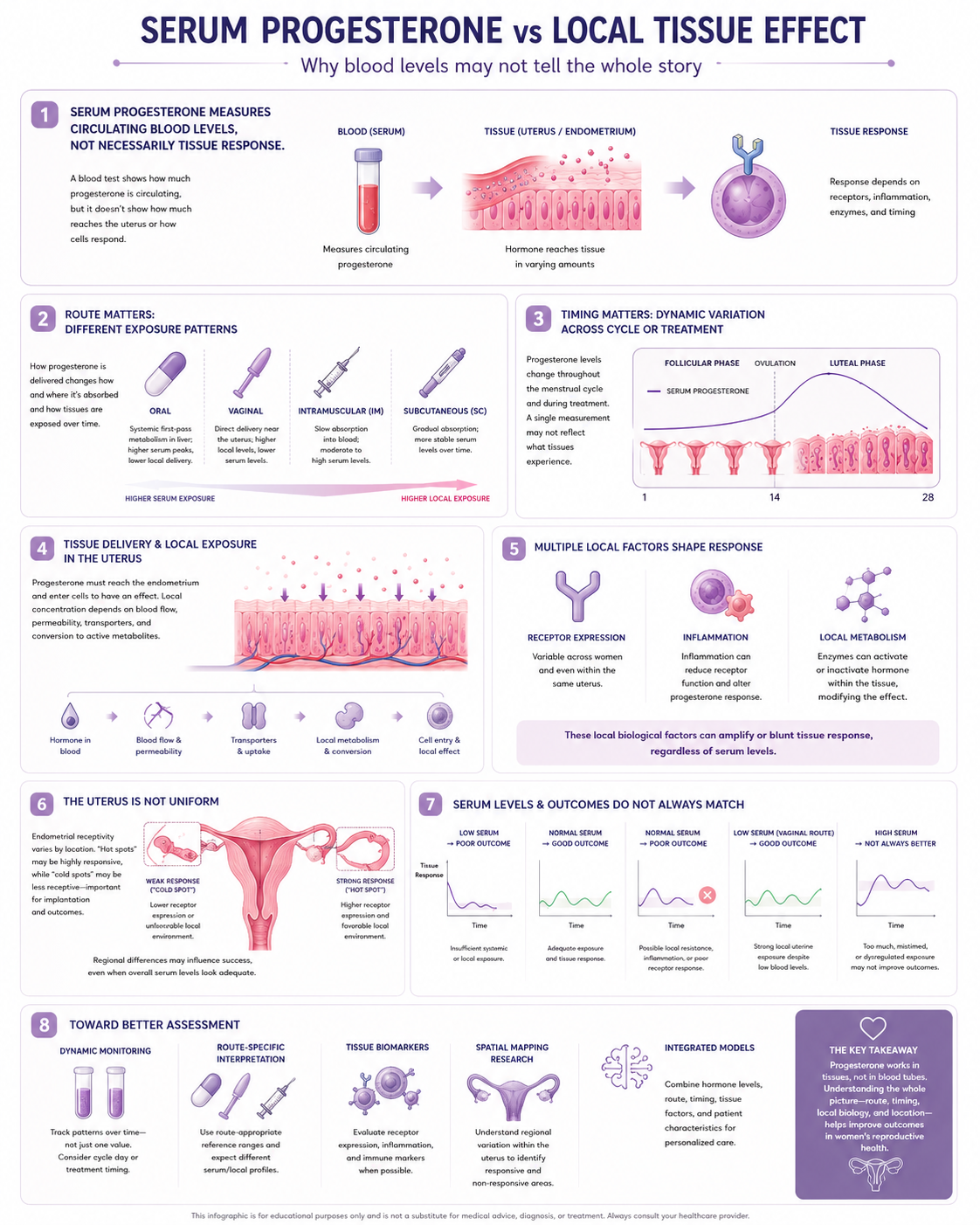
Progesterone is not supposed to act in the blood. It acts in tissues.
It acts in the endometrium, decidua, cervix, myometrium, placenta, immune cells, brain and other target tissues. A serum value can tell us what is circulating, but it does not automatically tell us how much progesterone reaches a specific tissue region, whether the receptors are present, whether inflammation changes the response, or whether the biological signal is strong enough in the right place at the right time.
This matters because progesterone research is full of mixed results.
Some studies suggest progesterone support improves outcomes in selected contexts. Others show weaker effects. Some routes appear similar in some settings but not in others. Some patients have low serum values and still do well. Others have apparently acceptable blood values but poor outcomes.
A serious progesterone discussion should therefore move beyond the simple question:
What is the progesterone level?
The better questions are:
When was it measured?
Which route was used?
What tissue needs the signal?
Does serum reflect local exposure?
Is the tissue responsive?
Is inflammation changing receptor function?
Are there local weak zones that a single average value cannot detect?
This article explains why progesterone may need to be understood as a dynamic, local and tissue-dependent signal, not only as a global blood number.
Serum progesterone: useful, but limited
Serum progesterone measures progesterone circulating in the blood.
It can be useful for:
- confirming ovulation
- assessing luteal phase function in some contexts
- monitoring IVF or frozen embryo transfer support
- identifying very low progesterone exposure
- evaluating timing in fertility treatment
- supporting clinical decision-making in selected protocols
In assisted reproduction, progesterone monitoring has become especially important in frozen embryo transfer and luteal support research. Reviews describe luteal phase support as central to IVF because ovarian stimulation and treatment protocols can disrupt natural luteal function, and progesterone supplementation is used to support implantation and early pregnancy.
However, a serum value is only one layer.
It does not directly measure endometrial progesterone concentration, receptor activation, gene expression, decidualization, immune tolerance or implantation readiness.
A blood value is a signal from the circulation.
It is not a full map of the uterus.
Progesterone is dynamic, not static
Progesterone is not biologically flat.
It changes across:
- the menstrual cycle
- the day after ovulation
- the implantation window
- early pregnancy
- IVF stimulation cycles
- frozen embryo transfer protocols
- medication timing
- route of administration
- absorption differences
- metabolism
- individual physiology
A single blood test is a snapshot.
That snapshot may be helpful, but it may not capture the full pattern.
In fertility treatment, timing can be critical. A progesterone level may look different depending on whether it is measured before dose, after dose, near embryo transfer, during luteal support or after pregnancy has started.
This is why dynamic measurement may sometimes be more informative than one isolated value.
The future may not be only “progesterone level.”
It may be “progesterone exposure over time.”
Serum level and tissue level are not always the same question
A key issue is whether serum progesterone reflects progesterone inside the endometrium.
Research has directly examined this question. One study in Human Reproduction noted that serum progesterone reflects progesterone in the vasculature, but it remains unclear whether systemic or endometrial progesterone levels are more important for determining endometrial receptivity.
That is a very important point.
The clinical habit is often to use blood as a proxy for tissue effect. But the uterus is not simply a passive recipient of whatever is in the bloodstream.
Tissue exposure may depend on:
- route of administration
- vascular delivery
- local diffusion
- uterine first-pass effects
- receptor expression
- local metabolism
- inflammation
- tissue thickness
- endometrial structure
- lesion-related disruption
- timing relative to implantation
So serum progesterone can be clinically useful while still being incomplete.
Both statements can be true.
Vaginal progesterone and the local uterine effect
Vaginal progesterone is especially interesting because it may produce local uterine exposure that does not always look the same as systemic exposure.
This is sometimes discussed as a uterine first-pass effect, where vaginal administration may deliver progesterone preferentially to the uterus compared with what serum values alone suggest.
That does not mean serum values are irrelevant.
It means route changes interpretation.
A serum level after vaginal progesterone may not mean the same thing as a serum level after intramuscular or subcutaneous progesterone. The tissue distribution can differ.
This is one reason why comparing progesterone routes is complicated. A lower serum level with one route does not always mean lower endometrial exposure. A higher serum level with another route does not automatically prove better local tissue effect.
Route is not just convenience.
Route is biology.
Why route matters
Different routes create different pharmacokinetic and tissue patterns.
Oral progesterone
Oral progesterone is metabolized through the liver. This can produce metabolites that may contribute to systemic effects such as sedation. Oral dosing may be useful in some contexts but is not equivalent to every other route.
Vaginal progesterone
Vaginal progesterone may create strong local uterine exposure, but serum values may be lower or harder to interpret. Absorption may vary between individuals.
Intramuscular progesterone
Intramuscular progesterone can create higher systemic levels and more stable circulating exposure, but may cause injection-related discomfort and has different distribution dynamics.
Subcutaneous progesterone
Subcutaneous progesterone offers another systemic route and is studied in luteal support settings.
Intrauterine progestin delivery
Intrauterine progestin systems can create strong local endometrial effects with lower systemic exposure, but this is a different clinical context from pregnancy support.
The key point:
A progesterone result must be interpreted through route.
The same number does not necessarily mean the same biological effect.
What IVF research is starting to ask
IVF and frozen embryo transfer research increasingly asks whether progesterone should be individualized.
Some studies and protocols examine whether low serum progesterone on the day of embryo transfer is associated with lower outcomes and whether rescue supplementation can improve results. One trial protocol describes serum progesterone monitoring in frozen embryo transfer cycles as an active research focus, with low levels on the day of transfer presumed to negatively affect outcomes and supplementation being tested.
Other studies have explored individualized luteal phase support based on serum progesterone levels, with some evidence suggesting that rescue strategies may help patients with low progesterone reach outcomes more similar to those with higher levels.
This is important because it shows a movement away from one-size-fits-all dosing.
But it also highlights a limitation:
Most individualized strategies still use serum progesterone as the main measurable variable.
That may be the best practical tool available today, but it may not be the final model.
The problem with average exposure
Medicine often uses averages.
Average serum level.
Average dose.
Average trial outcome.
Average patient response.
But reproductive tissues are spatially complex.
The uterus is not a uniform surface. The endometrium may vary regionally. Inflammation may be local. Receptor expression may vary. Adenomyosis, endometriosis, scarring, vascular differences or implantation-site biology may create uneven tissue response.
This raises an important research question:
Can a global blood value miss local areas of insufficient progesterone effect?
This is not established clinical practice.
But it is a serious first-principles question.
If progesterone needs to support a tissue process, and if the tissue response is uneven, then average exposure may not be enough to understand functional outcome.
Proposed research model: progesterone as a spatial tissue-coverage problem
This section is a proposed model, not established clinical guidance.
Current clinical practice often treats progesterone exposure as if a systemic or vaginal dose creates adequate biological coverage of the reproductive tissue.
But what if the problem is spatial?
Imagine that most of the endometrium receives enough progesterone signal, but a small region has poor response because of inflammation, receptor downregulation, altered blood flow, fibrosis, local immune activation or lesion-related disruption.
That local weak zone might still matter.
In other fields of medicine, local failure zones can be critical. A small area of poorly controlled tissue biology can influence the success of a larger treatment strategy. The analogy is not perfect, but the principle is useful:
A biological system may fail locally even when the average looks acceptable.
Applied to progesterone, this suggests possible future research questions:
- Are there regional differences in progesterone receptor expression?
- Do inflammatory “hot spots” respond differently to progesterone?
- Does endometriosis or adenomyosis create local low-response zones?
- Can endometrial biopsies from different regions show different progesterone response markers?
- Does vaginal progesterone create uneven local concentration gradients?
- Could tissue geometry influence required dose, route or timing?
- Can spatial transcriptomics map progesterone response more accurately?
This is not an argument that progesterone is a miracle treatment.
It is an argument that if progesterone matters, the way we measure and deliver it may need to become more precise.
Hot spots, weak zones and tissue response
The idea of a “hot spot” is useful if it is handled carefully.
A hot spot could mean a local region with:
- increased inflammation
- reduced progesterone receptor expression
- altered decidualization
- poor vascular delivery
- fibrosis
- immune activation
- abnormal local estrogen activity
- tissue injury
- endometriosis- or adenomyosis-related disruption
If such regions exist, they may help explain why some patients do not respond as expected to standard treatment.
But this is not yet routine clinical mapping.
Today, clinicians usually do not biopsy many geometrical regions of the uterus to map progesterone response. They do not routinely generate a spatial progesterone-responsiveness map. They do not calculate a geometric coverage model for vaginal or systemic progesterone exposure.
That does not mean the idea is wrong.
It means it belongs in research.
Why meta-analyses may not answer first-principles questions
Meta-analyses can be valuable.
But they can also hide biological heterogeneity.
If studies combine different patient groups, routes, doses, timings, indications and outcome measures, the average result may not tell us which mechanism matters.
A progesterone trial may include patients with:
- low circulating progesterone
- normal serum progesterone but poor tissue response
- inflammation-related implantation problems
- embryo chromosomal issues
- adenomyosis
- cervical insufficiency
- unrelated miscarriage mechanisms
- different medication absorption patterns
If all are grouped together, the result may look modest or inconsistent.
This does not mean meta-analysis is bad science.
It means meta-analysis cannot replace mechanism-based thinking.
Both are needed.
Population evidence tells us whether something tends to work.
First-principles biology asks why, where and for whom it might work.
Why this matters for patients
Patients often hear simple messages:
“Your progesterone is fine.”
“Your progesterone is low.”
“Take progesterone.”
“Progesterone does not help.”
“Vaginal progesterone gives local effect.”
“Blood levels do not matter.”
“Blood levels matter a lot.”
All of these may be partly true in certain contexts.
But the real answer is usually more conditional.
Progesterone interpretation depends on:
- cycle or pregnancy stage
- route of administration
- timing of measurement
- IVF or natural conception context
- clinical indication
- tissue responsiveness
- inflammation
- endometriosis or adenomyosis
- ultrasound findings
- pregnancy history
- outcome being targeted
Patients deserve a more mature explanation.
Not more certainty than the evidence allows, but more coherence.
What better progesterone monitoring might look like
Future progesterone research and care may move toward a layered model.
Layer 1: Dynamic serum measurements
Instead of one value, measure patterns over time in selected contexts.
Layer 2: Route-specific interpretation
Interpret serum values differently depending on vaginal, intramuscular, subcutaneous or oral administration.
Layer 3: Tissue response biomarkers
Study endometrial or decidual markers of progesterone action.
Layer 4: Inflammation and receptor context
Assess whether inflammation, endometriosis, adenomyosis or other conditions alter tissue response.
Layer 5: Spatial mapping
Use biopsy mapping, imaging, spatial transcriptomics or molecular profiling to identify local differences in tissue responsiveness.
Layer 6: Outcome-linked models
Connect hormone patterns, tissue response, embryo quality, implantation and pregnancy outcomes.
This is not standard care today.
But it may be where precision reproductive endocrinology should go.
What we should not claim
This topic can easily become overinterpreted.
We should not claim:
- serum progesterone is useless
- tissue levels are all that matter
- vaginal progesterone always gives adequate uterine effect
- higher dose is always better
- every failure is caused by local progesterone resistance
- biopsies should be performed routinely everywhere
- one hot spot model explains all infertility or miscarriage
- progesterone can solve all implantation problems
Those claims would be too strong.
A responsible position is:
Serum progesterone is useful but incomplete. Tissue effect depends on route, timing, local biology and tissue response. Better models are needed to understand when serum values are enough and when they miss important local biology.
Key message
Progesterone should not be understood only as a blood number.
Serum progesterone is useful, but progesterone acts in tissues. Local exposure, receptor response, timing, route, inflammation and tissue geometry may all shape the final biological effect.
The future of progesterone biology may require better measurement and spatial thinking.
Not because progesterone is a miracle medicine.
Because if a hormone signal matters, we should understand where it goes, when it arrives and whether the tissue can actually respond.
- Analysis of serum and endometrial progesterone in determining endometrial receptivity Human Reproduction / Oxford Academic
Study discussing the relationship between serum and endometrial progesterone and whether systemic or endometrial progesterone is more important for receptivity. - Luteal phase support in assisted reproductive technology Nature Reviews Endocrinology
Review of luteal phase physiology and luteal support in IVF, including why progesterone supplementation is used. - Initiating luteal phase support with subcutaneous progesterone based on low serum progesterone levels on embryo transfer day NIH PMC
Trial protocol showing that serum progesterone monitoring and rescue supplementation in frozen embryo transfer cycles are active research areas. - Comparison of Individualized Rescue Luteal Phase Support Strategies for Low Progesterone Levels NIH PMC
Study suggesting individualized luteal support based on serum progesterone on embryo transfer day may improve outcomes in selected FET cycles. - The Impact of Progesterone Administration Routes on Endometrial Receptivity in ART Cycles NIH PMC
Study comparing progesterone administration routes and endometrial receptivity assessment in IVF cycles.
